By: Debra A. Kent, PharmD, DABAT, FAACT
Out of Sight and Locked Up Tight: Pediatric pharmaceutical poisoning
Issue: BCMJ,
vol. 55, No. 1, January February 2013,
Page 33 BC Centre for Disease Control
Each year, over 25 000 poisonings are reported to the BC Drug and Poison Information Centre (DPIC) and nearly half of these involve children. In the first 11 months of 2012, DPIC was consulted on 10 008 cases involving children less than 6 years old.1 While 95% developed no toxicity or only minimal symptoms, 99 cases (< 1%) had moderate or major outcomes.[1]
A recent review of poisonings in the US reported that after years of pediatric pharmaceutical poisonings steadily declining, from 2001 to 2008 there was a statistically significant increase in pediatric pharmaceutical exposures, emergency room visits, and hospitalizations.[2] During this period, the number of adults taking five or more prescription medications rose from 7% to 11%.[2] This trend of increased pediatric pharmaceutical poisonings can also be predicted for Canada as the number of prescriptions in Canada grows by nearly 5% annually.[3]
Many factors contribute to pediatric poisoning and prevention efforts are targeted at high-risk circumstances and patients most at risk. Poisoning situations in young children are mostly unintentional and are a function of the child’s developmental stage. Toddlers and climbers between the ages of 1 to 3 years have the highest rate of poisoning.[1,4]
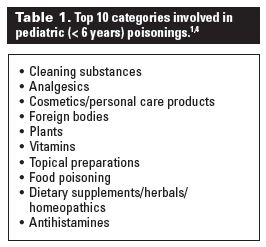
The substances commonly involved are those that are most accessible in their environment (Table 1).[1,4] However, the most common substances are not necessarily the most toxic. For example, children’s acetaminophen preparations are commonly ingested by young children, but the product strength and doses per bottle limit toxicity. Serious toxicity, however, can result when a child ingests an adult-strength, high-potency opioid analgesic such as fentanyl, methadone, or oxycodone (Table 2).[2,4] A single adult dose of these opioids is a potentially fatal dose for a toddler.
{kind=link}
{kind=link}
In the aforementioned US study, oral hypoglycemic agents accounted for the highest admission rate in children younger than 6 years of age, whereas death was most frequently related to unintentional ingestion of opioid analgesics, cardiovascular agents, and CNS drugs including sedatives/hypnotics/antipsychotics/antidepressants.[2]
As manufacturers strive to increase compliance in their patients on complex drug regimens, once-a-day sustained-release preparations contain potentially lethal amounts if ingested by a toddler (e.g., bupropion XL, verapamil SR, gliclazide MR). In addition, studies have shown that grandparents’ medications are involved in 10% to 20% of poisoning exposures in young children as these medications are often stored in blister packs or dosettes, which are not child-resistant.[2,5]
Poison prevention education activities have focused on pediatric poisoning for decades and, as a result, the mortality rate in children from unintentional poisoning has declined dramatically. However, pediatric poisoning from prescription pharmaceuticals appears to be increasing. As more medications are being prescribed, ongoing education efforts need to be directed toward parents, grandparents, prescribers, and pharmacists.
Poison Prevention Week (17–23 March) will highlight the problem and prevention of pediatric pharmaceutical poisoning with the theme “Out of Sight and Locked Up Tight.” Prevention materials and resources are available by contacting the BC Drug and Poison Information Centre at www.dpic.org.
—Debra A. Kent, PharmD, DABAT, FAACT
Clinical Supervisor, BC Drug and Poison Information Centre, BC Centre for Disease Control
Clinical Professor, Faculty of Pharmaceutical Sciences, University of British Columbia
References
1. Annual poisoning statistics, 1 January–30 November 2012. Vancouver, BC: BC Drug and Poison Information Centre.
2. Bond GR, Woodward RW, Ho M. The growing impact of pediatric pharmaceutical poisoning. J Pediatr 2012;160:265-270.
3. Canadian pharma sales shrink for first time in 30 years; number of prescriptions filled grows nearly 5%. IMS Health. 6 June 2012. Accessed 15 December 2012. www.imshealth.com/portal/site/ims/menuitem.856807fe5773bfb9ec895c973208c22a/?vgnextoid=4eb65890d33ee210VgnVCM10000071812ca2RCRD&vgnextfmt=default.
4. Bronstein AC, Spyker DA, Cantilena LR, et al. 2010 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 28th Annual Report. Clin Toxicol 2011;49:910-941.
5. McFee RB, Caraccio TR. “Hang up your pocketbook”—an easy intervention for the granny syndrome: Grandparents as a risk factor in unintentional pediatric exposures to pharmaceuticals. J Am Osteopath Assoc 2006;106:405-411.