Pharmacological management of stable chronic obstructive pulmonary disease
Issue: BCMJ,
vol. 50 , No. 2 , March 2008 ,
Pages 85 Clinical Articles
COPD is preventable and readily treatable. Pharmacological management includes interventions to promote smoking cessation (e.g., nicotine replacement therapy and non-nicotine drug therapy), domiciliary oxygen therapy for patients who are hypoxemic at rest, and long-acting bronchodilators with or without inhaled corticosteroids. For patients with mild disease and infrequent exacerbations, therapy with short-acting bronchodilators is the current standard. For more symptomatic patients, long-acting bronchodilators are needed to attenuate symptoms and reduce exacerbations. Patients who experience frequent exacerbations while using long-acting bronchodilators may require the addition of inhaled corticosteroids to improve health outcomes. Patients with severe or very severe disease may require therapy consisting of tiotropium, an inhaled corticosteroid, and a long-acting ß2 agonist.
Once the severity of a patient’s COPD has been quantified by spirometry, appropriate agents—including bronchodilators and inhaled corticosteroids—can be prescribed.
Chronic obstructive pulmonary disease (COPD) is the leading cause of hospitalization and one of the leading causes of mortality in BC.[1] Fortunately, stable COPD is readily treatable. Management of patients exhibiting chest symptoms (Table 1) should begin with spirometry, which can often be done in an office setting. The spirometry measurements can then be used to quantify COPD severity according to guidelines from the Canadian Thoracic Society, the American Thoracic Society, and the European Respiratory Society (Table 2).[2,3]
Accurate staging requires at least three technically acceptable, irregularity-free spirograms consisting of expiratory efforts of at least 6 seconds. Additionally, the difference between the two largest measurements of FEV1 (forced expiratory volume in 1 second) and FVC (forced vital capacity) should be within 0.2 L. COPD is indicated by spirometry if the FEV1 to FVC ratio postbronchodilator (e.g., after 400 ug of salbutamol [Ventolin]) is 0.7 L or less.
Severity of COPD is established by a postbronchodilator measurement of FEV1 as a percentage of predicted normal. Mild is defined as an FEV1 that is 80% of predicted or greater; moderate is defined as an FEV1 between 50% and 80% of predicted; severe is defined as an FEV1 between 30% and 50% of predicted; and very severe is defined as an FEV1 less than 30% of predicted.
Once the severity of the patients’ COPD has been quantified, then management approaches can be considered (Table 3). Smoking cessation is recommended for all patients regardless of severity. Vaccination for influenza (every year) and for pneumococcal pneumonia (every 5 to 10 years) is recommended for all patients unless specific contraindications exist.
For patients with mild and periodic symptoms, short-acting bronchodilators such as salbutamol can be used either intermittently or on a regular basis for symptomatic relief of dyspnea. Patients with moderate to moderately severe disease can use a long-acting bronchodilator. This can be either an anticholinergic agent such as tiotropium or a ß2 agonist such as salmeterol or formoterol.
Patients who have more than one exacerbation per year requiring oral corticosteroids and/or antibiotics should have inhaled corticosteroids added to a long-acting bronchodilator to reduce exacerbation rates and improve health status. Patients with severe or very severe disease may require the regular use of a long-acting ß2 agonist/inhaled corticosteroid combination in conjunction with tiotropium.[4]
Clinical scenarios
Management of mild COPD: Patient 1
A 65-year-old man presents with an early morning cough that has bothered him for the past year. The cough is usually productive of mucoid sputum. There is no hemoptysis. He is a current smoker with a 25-pack-a-year smoking history. He has smoked half-a-pack per day, on average, since 15 years of age. Although he admits that for the past 3 years he has been having more chest colds, which can last 2 to 3 weeks at a time, he feels well in general and has remained asymptomatic in his daily activities.
He has no significant occupational history. There is no history of allergy, asthma, sinusitis, or respiratory infections in his early childhood. There is no family history of asthma or COPD. He has had no previous hospitalizations for any respiratory problems. He has no comorbidities. The physical examination is normal. How should this patient be managed?
With the patient’s history of smoking and symptoms of cough and sputum production, you suspect that he has COPD. The next step is to obtain lung function measurements to support your diagnosis and to assess the degree of severity of the airflow limitation, which can help guide treatment and assist with a prognosis.
When spirometry is performed on this patient, his postbronchodilator FEV1is 3.0 L (or 87% of predicted) and his FVC is 4.41 L (or 94% of predicted). The FEV1 to FVC ratio is 0.68 (or 75% of predicted). Although both FEV1 and FVC are in the “normal” range, the reduced FEV1 to FVC ratio (especially in the presence of an appropriate smoking history and symptoms) objectively confirms a diagnosis of COPD.[2] The patient’s post-bronchodilator FEV1 of greater than 80% of predicted indicates that he has mild COPD.[1]
Smoking cessation: This is the most important intervention for this patient. The family physician should counsel the patient to stop smoking and consider a referral to a smoking cessation clinic for additional support, such as with cognitive and behavioral therapy.[5]
Cognitive therapy can include techniques of distraction, positivism, relaxation, and mental imagery.[5] Behavioral interventions can include avoidance of triggers for smoking, such as alcohol or coffee, stress, and associations with other smokers.
Counseling is effective for about 22% of smokers, leading them to become sustained quitters.[6] Even a brief intervention in a physicians’ office can help 5% to 10% of smokers quit.[7] Drug therapy is often needed for the remaining smokers. Pharmacological therapies can be divided into two large groups: nicotine replacement therapy and non-nicotine drug therapy.
Nicotine replacement is usually provided as a patch, gum, or lozenges. The choice between these formulations is based on patient preference and smoking habits. High doses of nicotine replacement are more effective than lower doses but cause more side effects.[5] However, for those patients who do not respond to the lower doses, higher doses should be considered. Side effects include insomnia, skin irritation (for patches), and early morning cravings for nicotine.
Non-nicotine drug therapies include psychotropic medications such as bupropion (Zyban) and more recently α4ß2 nicotinic acetylcholine receptor agonists such as varenicline (Chantix).[8] Bupropion should be prescribed at least 1 week before the cessation date, so that adequate blood levels can be achieved, and then continued for 2 to 3 months following cessation. Bupropion is contraindicated in patients with a seizure disorder.[4]
Some patients experience insomnia and dry mouth. Bupropion can be used with nicotine replacement therapy. Success rates vary depending on the population but usually range between 10% to 40%. Varenicline shows great promise as an alternative to bupropion. A recent study indicates that cessation was achieved over 3 months in more than 40% of smokers (compared with bupropion, which achieved a cessation rate of 30%).
At 1 year, smokers taking varenicline had higher cessation rates than those who took bupropion (23% versus 14%).[8-10]
Other therapies: In addition to smoking-cessation therapy, the patient should also receive vaccine for pneumococcal pneumonia every 5 to 10 years (a recommendation that applies especially to COPD patients 65 years or older) and yearly influenza vaccination unless contraindications exist.
If the patient remains symptomatic despite smoking cessation, treatment with a short-acting bronchodilator is needed. The short-acting bronchodilators can be given on an as-needed basis if the patient has periodic symptoms, or around the clock if the patient has persistent symptoms.
In most cases patients will respond to either an inhaled short-acting ß2 agonist such as salmbulerol or an anticholinergic such as ipratropium by itself. However, with persistent symptoms, a combination of the two may be necessary.[11]
Management of moderate COPD: Patient 2
A 72-year-old woman has moderate COPD that was diagnosed 5 years earlier. Upon presentation her FEV1 is 1.5 L or 54% of predicted. She has managed to stop smoking. Although she is taking combination bronchodilator therapy (salbutamol and ipratropium), two puffs four times per day, she is still short of breath when walking more than 100 m or cleaning the house. What additional treatments are needed?
In this patient, short-acting bronchodilators are no longer able to fully control her symptoms. The currently available evidence indicates that long-acting ß2 agonists and long-acting anticholinergics improve respiratory symptoms and reduce the risk of exacerbations beyond that achieved by short-acting bronchodilators.[11]
There is, however, insufficient evidence to recommend one class of long-acting bronchodilators over another class. There is a growing body of evidence that inhaled corticosteroids in combination with a long-acting ß2 agonist benefit COPD patients who have an FEV1 of less than 60% of predicted by reducing the rate of exacerbations and improving health status.[12]
Monotherapy with tiotropium may be just as effective as a combination of salmeterol and fluticasone in reducing exacerbations in patients with moderate disease.[4] However, one large randomized controlled trial indicates that tiotropium is also associated with increased mortality compared with combination therapy.[13]
A 2-year randomized controlled trial (sponsored by GlaxoSmithKline) of 1323 patients with an FEV1 between 50% and 80% of predicted showed no differences in the exacerbation rate between tiotropium and salmeterol/fluticasone combination. However, patients in the salmeterol/fluticasone arm had better quality of life and experienced 44% fewer deaths than patients taking tiotropium.[13]
Thus, for this patient with moderate COPD, in addition to vaccination for influenza and pneumococcal pneumonia and short-acting bronchodilators, a combination therapy with inhaled corticosteroid and a long-acting ß2 agonist can be provided. The alternative would be to use tiotropium in lieu of the combination therapy.
Management of severe COPD: Patient 3
A 70-year-old man who has had very severe COPD for 13 years has an FEV1 of 0.9 L (30% of predicted). He is on a number of medications, including short-acting ß2 agonists, ipratropium bromide, and an inhaled corticosteroid. He stopped smoking 2 years ago but he has dyspnea at rest even on these medications.
He has had two hospitalizations for COPD in the last 5 years and needed oral corticosteroids on two different occasions over the past year. What pharmacological treatment should be recommended for this patient?
The recently published large randomized trials have shed tremendous light on the treatment of patients with severe COPD.[4,12]
Monotherapy with inhaled corticosteroids is clearly inferior to combination therapy with an inhaled corticosteroid and a long-acting ß2 agonist.[12] Over 3 years, combination therapy would be expected to reduce exacerbations by 25% compared with placebo, whereas a long-acting ß2 agonist and an inhaled corticosteroid would be expected to reduce exacerbation by 15% and 18%, respectively.[12]
Tiotropium is also effective in reducing exacerbations in the short term. However, the Canadian Optimal Study showed that over 1 year, adding combination therapy to tiotropium reduced the rate of hospitalization for COPD by 47% compared with tiotropium alone.[4] Moreover, patients taking combination therapy and tiotropium had better quality of life and improved lung function compared with patients taking tiotropium alone.[4]
Taken together, these data indicate that for patients with severe COPD (FEV1 less than 50% of predicted) and with recurrent exacerbations, tiotropium in conjunction with a combination of inhaled corticosteroid and long-acting ß2 agonist should be considered.
At this time, long-term oral corticosteroid therapy is generally not recommended because of potential side effects. Oral corticosteroids should be reserved for short-term use during exacerbations. Oral theophyllines have fallen out of favor in recent years owing to their narrow therapeutic range and toxicity profile. In general, most patients can be managed without oral theophyllines; however, in patients whose symptoms are refractory to a combination therapy that includes an inhaled corticosteroid, long-acting ß2 agonist, and tiotropium, oral theophyllines may be considered.
For those who are prescribed oral theophyllines, close follow-up is needed (along with blood level monitoring) to ensure toxicity does not develop.
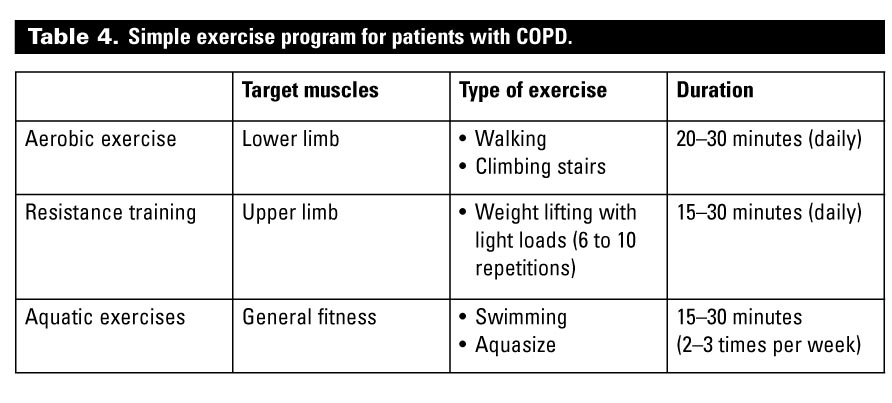
For patients with severe, moderate, or mild COPD, drug therapy should be provided in concert with nonpharmacological therapies. This includes exercise training, which in many cases can be performed at home (Table 4).
Conclusions
With the recent improved understanding of the pathogenesis of COPD, primary preventions provide the best hope to control the rapid rise of this disease.
Smoking cessation is the cornerstone of management and therapy with bronchodilators is the first-line pharmacological therapy for symptomatic patients. For more advanced disease states, a combination of inhaled corticosteroid and long-acting ß2 agonist should be considered.
For patients with mild to moderate COPD and infrequent exacerbations, tiotropium or a long-acting ß2 agonist is likely sufficient. However, for severe or very severe COPD, combination therapy is usually required, and for patients with persistent symptoms and frequent exacerbations requiring hospitalizations, a combination of inhaled corticosteroid, long-acting ß2 agonist, and tiotropium may be needed for optimal outcomes.
Competing interests
Dr Sin has received honoraria for speaking from GlaxoSmithKline (GSK), research funding from GSK, AstraZeneca, and Boehringer Ingelheim, and served as a consultant to GSK and AstraZeneca.
References
1. Hospital crunch. Vancouver Sun, 30 May 2007.
2. O’Donnell DE, Aaron S, Bourbeau J, et al. State of the Art Compendium: Canadian Thoracic Society recommendations for the management of chronic obstructive pulmonary disease. Can Respir J 2004;11 suppl B:7B-59B.
3. Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J 2005;26:948-968.
4. Aaron SD, Vandemheen KL, Fergusson D, et al. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease: A randomized trial. Ann Intern Med 2007;146:545-555.
5. Schroeder SA. What to do with a patient who smokes. JAMA 2005;294:482-487.
6. Kanner RE, Connett JE, Williams DE, et al. Effects of randomized assignment to a smoking cessation intervention and changes in smoking habits on respiratory symptoms in smokers with early chronic obstructive pulmonary disease: The Lung Health Study. Am J Med 1999;106:410-416.
7. Bailey WC. Smoking cessation. Chest 1985;88:322-324.
8. Gonzales D, Rennard SI, Nides M, et al. Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: A randomized controlled trial. JAMA 2006;296:47-55.
9. Jorenby DE, Hays JT, Rigotti NA, et al. Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: A randomized controlled trial. JAMA 2006;296:56-63.
10. Tonstad S, Tonnesen P, Hajek P, et al. Effect of maintenance therapy with varenicline on smoking cessation: A randomized controlled trial. JAMA 2006;296:64-71.
11. Sin DD, McAlister FA, Man SF, et al. Contemporary management of chronic obstructive pulmonary disease: Scientific review. JAMA 2003;290:2301-2312.
12. Calverley PM, Anderson JA, Celli B, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med 2007;356:775-789.
13. Wedzicha JA, Calverley PM, Seemungal TA, et al. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am J Respir Crit Care Med 2008;177:19-26.
Dr Sin is an associate professor in the Department of Medicine at the University of British Columbia and a staff respirologist at St. Paul’s Hospital and a Canada Research Chair in COPD.
{kind=link}
{kind=link}
{kind=link}