
Total mesorectal excision outcomes--The Dutch trial
Issue: BCMJ,
vol. 45 , No. 7 , September 2003 ,
Pages 314-318 Clinical Articles
One of the major problems in the treatment of rectal cancer has been the inability to achieve local control. The conventional surgical procedure, which involves blunt digital dissection, is associated with a high incidence of local recurrence.
In an attempt to improve local control and survival, many adjuvant treatment modalities have been investigated. In the context of conventional non-standardized surgical procedures, preoperative radiotherapy has shown to improve local control and overall survival.
In recent years treatment outcome has been extensively improved by the introduction of the total mesorectal excision (TME) technique. This surgical technique resulted in such low recurrence rates and improved survival that the question had to be answered whether preoperative short-term radiotherapy is still beneficial in TME-treated patients. This question was answered in the TME trial set up by the Dutch ColoRectal Cancer Group that randomized between standardized and quality-controlled TME surgery alone and TME surgery preceded by short-term preoperative radiotherapy.
This paper reviews the developments in the treatment of resectable rectal cancer, highlights the results from the Dutch TME trial, and considers future directions in improving outcome.
Total mesorectal excision has become the new standard of operative rectal cancer management. Here, the lead investigator of the ground-breaking Dutch trial discusses the findings.
Local recurrence: A major problem in rectal cancer
Local recurrence is a serious problem in the treatment of rectal cancer.[1] It causes severe disabling symptoms that are difficult to treat and often kill the patient. The basic conventional procedure that involves blunt dissection of the rectal fascia fails to remove all mesorectal tissue, which causes high recurrence rates from 15% to 45%.[2] Additional radiotherapy has been given in an attempt to improve local control after conventional surgery. Results of the studies that investigated the role of radiotherapy showed that preoperative radiotherapy is more effective than postoperative radiotherapy in reducing local recurrence rates.[3] The Swedish Rectal Cancer Trial found that preoperative radiotherapy also improved the rate of survival at 5 years.[4] The results of a large meta-analysis[5] strengthened the idea that the combination of preoperative radiotherapy and surgery could improve overall and cancer-specific survival compared with surgery alone.
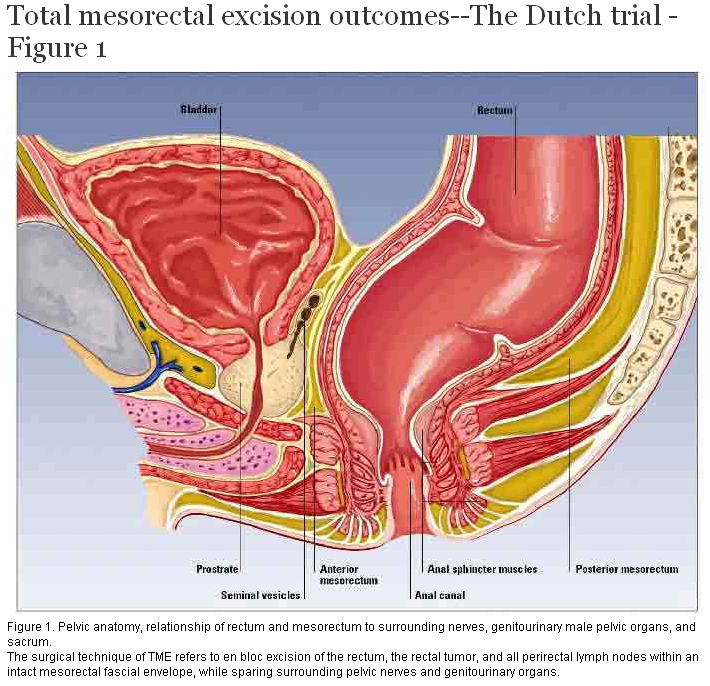
The acknowledgment of the important role of circumferential margin involvement in the occurrence of local recurrences has led to the introduction of total mesorectal excision (TME) surgery. The concept of TME was introduced by Heald at the North Hampshire Hospital in Basingstoke in 1979.[6] By using sharp dissection under direct vision, a relatively bloodless plane is followed along the outer surface of the rectum (Figure 1). This technique ensures a specimen with intact mesorectum with negative tumor margins in the majority of resectable (i.e., mobile) rectal cancers. Heald’s first series of 122 curative anterior resections showed a cumulative risk of local recurrence at 5 years of 2.7% and overall corrected survival of 87.5% at 5 years.[7] These excellent results were matched in Enker’s personal series of 246 curable Dukes’ stage B and C patients, of which only 18 developed a local recurrence. The actuarial cancer-specific 5-year survival was 74.2%.[8] Aitken published a study on a series of 64 patients who underwent a curative TME procedure: only one patient (1.6%) developed a local recurrence.[9]
{kind=link}
Since the introduction of TME surgery has resulted in such low recurrence rates and improved survival, the question of whether adjuvant treatment is still capable of achieving any further improvement in outcome had to be answered. As the skills and experience of the surgeon and the surgical technique are of major importance in achieving local control,[10] standardization and quality control with respect to surgery is indispensable for evaluating the effects of adjuvant treatment.
The Dutch ColoRectal Cancer Group, the Nordic Gastro Intestinal Tumour Adjuvant Therapy, and the European Organization for Research and Treatment of Cancer (EORTC) jointly organized a large prospective randomized multicentre trial to investigate the efficacy of preoperative radiotherapy (five fractions of 5 Gy) in combination with standardized total mesorectal excision in patients with rectal cancer. Standardization and quality control of surgery, radiotherapy, and pathology were achieved by means of a monitoring committee of specially trained instructor surgeons, a panel of supervising pathologists, and study coordinators for surgery, radiotherapy, and pathology.
Eligibility criteria included histologically confirmed adenocarcinoma of the rectum without evidence of distant metastases. The inferior margin of the tumor had to be located not further than 15 centimetres from the anal verge and below the level of S1-2. Patients with fixed tumors were excluded, as were patients with locally treated (transanal resected) tumors.
Patients were enrolled between January 1996 and December 2000. A total of 1861 patients were randomly assigned to one of the two treatment groups. There were 1530 patients from 84 Dutch hospitals, 228 patients from 13 Swedish hospitals, and 103 from 11 other European and Canadian centres. Of these 1861 patients, 56 were ineligible before randomization, including four patients for whom there was no information on eligibility. Of the 1805 eligible patients, 1653 had a curative resection. Of the remaining 152 patients, 57 did not undergo a macroscopically complete resection, and of 95 patients distant metastases were discovered during the surgical procedure.
Before the start of the TME trial, there were doubts whether the excellent results obtained by specialized surgeons could be matched in a large multicentre trial. To investigate this, we compared the outcome of the Dutch TME trial patients who did not receive preoperative radiotherapy with the results from a former randomized trial, the Cancer Recurrence and Blood Transfusion (CRAB) trial.[11] In this latter trial, conventional, nonstandardized surgery was performed. This analysis showed that introduction of TME had led to a substantially lower recurrence rate when only events within 2 years were analyzed: 16.3% in the CRAB trial vs 8.6% in the TME trial. With this low recurrence rate in the TME trial, it was made clear that good local control can be achieved by general surgeons after a thorough surgical instruction. These results are in concordance with the report of Martling and colleagues.[12] In this analysis a comparison was made between the Stockholm I and II randomized trials in which conventional surgery with or without radiotherapy was performed, and the TME project that introduced the concept of TME to surgeons in Stockholm; the 2-year local recurrence rates decreased from 14%–15% to 6%.
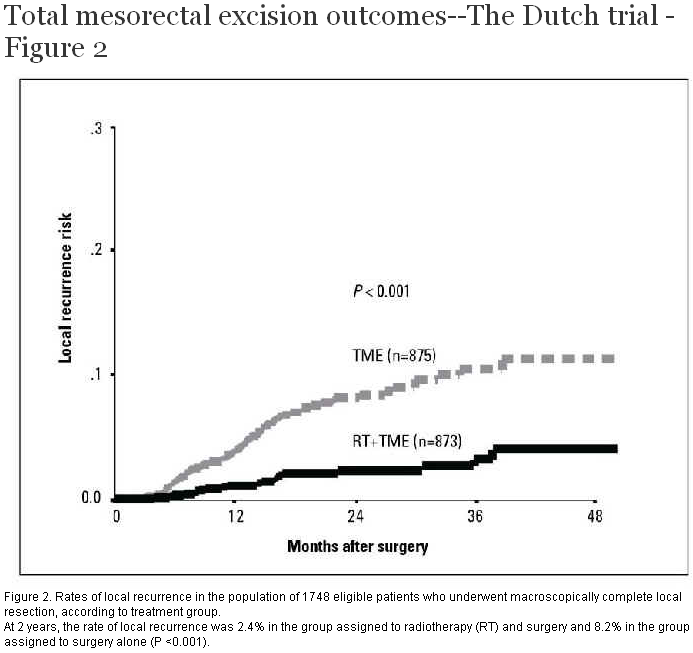
The local recurrence analysis for all patients of the TME trial showed a 2-year local recurrence rate of 5.3%. In the TME group this rate was 8.2% and in the radiotherapy plus TME group it was 2.4% (P <0.001) (see Figure 2). An effect of preoperative radiotherapy on overall survival could not be detected (see Figure 3). The beneficial effect of preoperative radiotherapy was observed for all tumor locations 15 centimetres or less from the anal verge and for all TNM stages. In a univariate subgroup analysis, however, this effect was not significant in patients who had lesions located more than 10 centimetres from the anal verge and in patients with TNM stage I and IV. Nevertheless, multivariate tests indicated that the beneficial treatment effect did not differ among subgroups defined according to tumor location, TNM stage, and treatment assignment. Therefore, the decision not to irradiate these patients should be made with reservation.
{kind=link}
{kind=link}
Based on experiences of former randomized trials,[13] concerns have been expressed about the side effects of hypofractionated radiation. In this trial, however, no significant differences with respect to postoperative morbidity and mortality were found other than an increase of perineal complications in the radiotherapy plus TME group in patients who had an abdominal perineal resection.
The successor to the Dutch TME-trial is the PROCTOR (Preoperative Radiotherapy and/or Adjuvant Chemotherapy Combined with TME Surgery in Operable Rectal Cancer) trial. So far, chemotherapy has shown to have little effect in combination with conventional surgery in the prevention of distant recurrences and improvement of survival. This may be explained partly by the high rate of local recurrence associated with conventional procedures that might have masked the beneficial effect of chemotherapy. The additional value of postoperative chemotherapy (5-fluorouracil/leucovorin according to Mayo or Nordic regimen) is now investigated in patients with stage II and III rectal cancer that had a R0-resection. The main objective is to examine whether postoperative chemotherapy leads to a substantial improvement in overall survival. The overall survival in the arm treated without chemotherapy is expected to be 60%. Assuming that postoperative chemotherapy leads to an improvement in overall survival from 60% to 70%, 500 patients are needed per arm. The secondary objective is to investigate the effect of chemotherapy on local and distant tumor control. This trial is open to accrual.
In recent decades, substantial progress has been made in the treatment of rectal cancer. New surgical techniques have played a major role in improving treatment outcome. Local control and survival have been improved by the TME technique. TME is accomplished by precise sharp dissection within the true pelvis around the integral mesentery under direct vision, enveloping the entire midrectum. Apart from the beneficial effect on local recurrence and survival, the TME dissection is also associated with a higher incidence of sphincter preservation and of pelvic and autonomic nerve preservation. This implies avoiding both colostomy and impotence, thus increasing patients’ quality of life. One side effect of the higher rate of sphincter-saving procedures, however, is the increased risk of anastomotic leakage.
To improve results of surgery, many adjuvant treatment regimens have been tested. The studies published so far, however, have been carried out without a clear definition of the surgical procedure to be followed and without sufficient quality control. In none of the trials were criteria formulated and controlled with respect to safety margins, excision of the mesorectum, and lymph node dissection. Currently, global local recurrence rates of less than 10% can be achieved with standardized TME surgery alone. The question, therefore, is whether a further improvement can be obtained by adjuvant therapy.
In this paper an overview was given on the efforts that have been made to reduce the local recurrence risk in patients with rectal cancer. Due to severe and disabling symptoms caused by local failure, local pelvic control is generally accepted as a main objective of any adjuvant treatment. The Dutch TME trial clearly showed that short-term preoperative radiotherapy could reduce the risk of local recurrence more than threefold in the setting of standardized TME surgery (8.2% vs 2.4% after a median follow-up of 2 years, P <0.001). In terms of tumor biology, preoperative radiotherapy is preferred to postoperative irradiation since tumor cells before surgery have higher oxygen saturation and are therefore more sensitive to irradiation. Furthermore, preoperative radiotherapy devitalises tumor cells that may be dispersed during the operation, and therefore reduces the risk of metastasis. On the other hand, postoperative radiotherapy allows exclusion of patients with rectal cancer stages Dukes’ A and D. To guarantee its effectiveness, postoperative irradiation should start no later than 4 to 6 weeks after surgery to prevent tumor cell proliferation in the postoperative, fibrous, and hypoxic tissues. However, many patients turn out not to be fully recovered from the operation at this time, which causes a delay in receiving the adjuvant radiotherapy. This lack of compliance therefore jeopardizes the possible benefits of postoperative radiotherapy.
The Dutch TME trial is one of the first trials that evaluated the role of adjuvant treatment in combination with TME surgery. Standardization of surgery, radiotherapy, and pathology was achieved. The accrual went quickly and the trial proved feasible. It was clearly shown that short-term preoperative radiotherapy has a beneficial effect in TME-treated patients.[14] Many aspects of this trial have been strictly quality controlled. There are extensive data on quality of life as well as a tumor bank of fresh-frozen material with a high potential for future micro-array analyses. This will enable the development of tailor-made treatment modalities in the future.
In the last 10 years, it has become clear that adjuvant treatment has the potential of decreasing local recurrence risk and improving overall survival. Total mesorectal excision has become the new standard of operative rectal cancer management. To preoperatively identify patients who will most likely benefit from (neo-) adjuvant therapy, emphasis needs to be put on better preoperative staging and imaging. Therefore, diagnostics and surgical treatment must be standardized in current and future trials to assess the value of adjuvant therapy in a reliable way.
Competing interests
None declared.
References
1. Wiggers T, de Vries MR, Veeze-Kuypers B. Surgery for local recurrence of rectal carcinoma. Dis Colon Rectum 1996;39:323-328. PubMed Abstract
2. MacFarlane JK, Ryall RD, Heald RJ. Mesorectal excision for rectal cancer. Lancet 1993;341:457-460. PubMed Abstract
3. Frykholm GJ, Glimelius B, Pahlman L. Preoperative or postoperative irradiation in adenocarcinoma of the rectum: Final treatment results of a randomized trial and an evaluation of late secondary effects. Dis Colon Rectum 1993;36:564-572. PubMed Abstract
4. Improved survival with preoperative radiotherapy in resectable rectal cancer. Swedish Rectal Cancer Trial. N Engl J Med 1997;336:980-987. PubMed Abstract Full Text
5. Camma C, Giunta M, Fiorica F, et al. Preoperative radiotherapy for resectable rectal cancer: A meta-analysis. JAMA 2000;284:1008-1015. PubMed Abstract Full Text
6. Heald RJ. A new approach to rectal cancer. Br J Hosp Med 1979;22:277-281. PubMed Citation
7. Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986;1:1479-1482. PubMed Abstract
8. Enker WE, Thaler HT, Cranor ML, et al. Total mesorectal excision in the operative treatment of carcinoma of the rectum. J Am Coll Surg 1995;181:335-346. PubMed Abstract
9. Aitken RJ. Mesorectal excision for rectal cancer. Br J Surg 1996;83:214-216. PubMed Abstract
10. Martling A, Cedermark B, Johansson H, et al. The surgeon as a prognostic factor after the introduction of total mesorectal excision in the treatment of rectal cancer. Br J Surg 2002;89:1008-1013. PubMed Abstract
11. Houbiers JG, Brand A, van de Watering LM, et al. Randomised controlled trial comparing transfusion of leucocyte-depleted or buffy-coat-depleted blood in surgery for colorectal cancer. Lancet 1994;344:573-578. PubMed Abstract
12. Martling AL, Holm T, Rutqvist LE, et al. Effect of a surgical training programme on outcome of rectal cancer in the County of Stockholm. Stockholm Colorectal Cancer Study Group, Basingstoke Bowel Cancer Research Project. Lancet 2000;356:93-96. PubMed Abstract Full Text
13. Cedermark B, Johansson H, Rutqvist LE, et al. The Stockholm I trial of preoperative short term radiotherapy in operable rectal carcinoma. A prospective randomized trial. Stockholm Colorectal Cancer Study Group. Cancer 1995;75:2269-2275.
14. Kapiteijn E, Marijnen CA, Nagtegaal ID, et al. Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer. N Engl J Med 2001;345:638-646. PubMed Abstract Full Text
C.J.H. van de Velde, MD, PhD, FRCS, FRCPS
On behalf of the Dutch ColoRectal Cancer Group
Dr van de Velde is chair of the Dutch ColoRectal Cancer Group at the Department of Surgery at Leiden University Medical Center, Leiden, the Netherlands.