Lipid-lowering treatment prevents first cardiovascular events in high-risk populations with normal or even low cholesterol level
Issue: BCMJ,
vol. 45 , No. 10 , December 2003 ,
Pages 515-519 Clinical Articles
In two large studies of lipid-lowering (ASCOT-LLA and MRC/BHF Heart Protection Study) therapy in primary prevention populations, there were highly significant reductions in cardiovascular events. These findings, together with a wealth of epidemiological, pathological and genetic information, make a strong argument for lipid-lowering treatment in high-risk populations. Calculated absolute risk reductions—while an important consideration—may underestimate the benefits of statin treatment in primary prevention.
The ASCOT-LLA and MRC/BHF Heart Protection Studies
Is there a place for statin treatment of patients at high risk for atherothrombotic events? The author argues that and clinical trial evidence supports it.
While many physicians (particularly the lipidologists!) accept dyslipidemia as one of the major risk factors for atherosclerosis, some remain skeptical about the role of lipids in atherogenesis. Their degree of skepticism may be lessened by the data from the recently reported Anglo Scandinavian Cardiac Outcomes Trial—Lipid Lowering Arm (ASCOT-LLA)[1] and MRC/BHF Heart Protection Study in people with diabetes.[2] Of more than 19 000 hypertensive patients, both men and women aged 40 to 79 years on two different anti-hypertensive regimens, 10 300 (81% men) with cholesterol (TC) concentrations below 6.5 mmol (average TC was 5.5 mmol/L, LDL-C 3.4 mmol/L and HDL-C 1.3 mmol/L) were assigned to either atorvastatin 10 mg or placebo treatment.
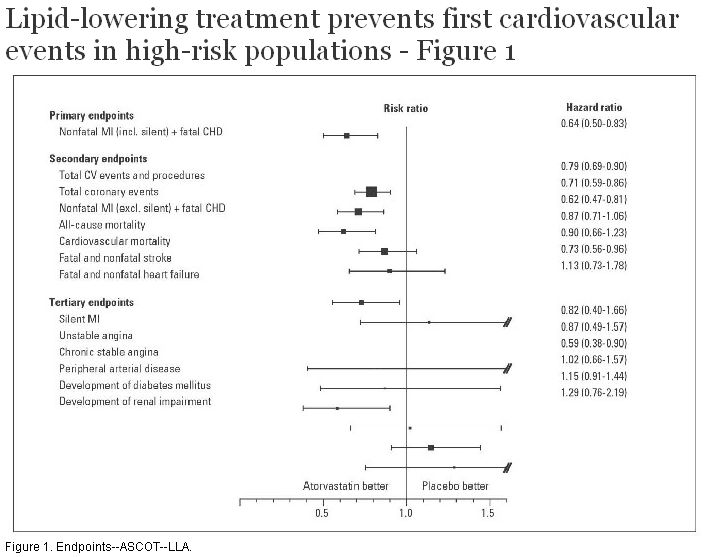
It should be pointed out that the trial participants had at least three other cardiovascular risk factors, such as age >65 years, male gender, smoking, diabetes, family history of early coronary disease, microalbuminuria, TC:HDL-C ratio >6.0, EKG abnormalities, or left ventricular hypertrophy. Because of significant differences in clinical outcomes between the atorvastatin treated group and the placebo treated group, the trial was stopped at 3.3 years follow-up instead of the planned 5 years. All of the following were significantly lower in the lipid lowering arm of the study (see Figure 1):
• Combined outcome of nonfatal myocardial infarction and fatal coronary artery disease was reduced by 36%.
• Fatal and nonfatal stroke was reduced by 27%.
• All cardiovascular events and procedures by 21% and all coronary events were reduced by 29%.
The overall mortality between the groups was not significantly different, though there was a trend toward lower mortality in the atorvastatin group (185 and 212 participants died in the atorvastatin and placebo arms, respectively). Of interest is the observation that some benefit already occurred in the first year of treatment when the total serum cholesterol was decreased by 1.3 mmol/L in the treatment group.
Two comments appeared recently regarding ASCOT-LLA. One[3] of them addresses the increased cardiovascular risk and difficulties in achieving ideal blood pressure in several ethnic groups, such as African-American patients, Afro-Caribbean patients, and, more pertinent to BC, patients of Southeast Asian origin. Thus, the criticism is that the trial participants from these ethnic groups may have had less than ideal blood pressure control and were therefore more likely to suffer the adverse consequences of hyperlipidemia. The author advocates a lower threshold for use of statins in these ethnic groups (he also includes individuals with metabolic Syndrome X). A plea is also made for multidrug therapy for hypertension in these ethnic groups. Another comment appeared recently in Canadian Medical Association Journal[4] and focuses on the possible underestimation of the degree of the benefit of atorvastatin. The confounders include a cross-over between the two groups that was 21% (i.e., 21% of the placebo group ended up using lipid-lowering medications) after 3 years of follow-up, the fact that the study was stopped nearly 2 years earlier than other statin trials, that blood pressure was aggressively treated in both patient groups, and that the dose of atorvastatin was not titrated from the starting dose of 10 mg per day. All these factors may have contributed to the relatively small absolute reduction in the first coronary event and the fact that only a trend toward the decrease in overall mortality was seen.
This study is important for a number of reasons. Once again stroke was significantly reduced in the treatment group, emphasizing that even in patients with good blood pressure control, lowering of cholesterol prevents both fatal and nonfatal stroke. In addition, the incidence of stroke was decreased in patients over 70 years of age—unlike PROSPER Trial.[5] Similar to the results of the Heart Protection Study,[6] the benefits of lipid-lowering treatment were observed across all baseline lipid levels.
In the recently published MRC/BHF Heart Protection study in people with diabetes,[2] there was a significant reduction of 33% in vascular events among 2912 diabetic participants who did not have any diagnosed arterial disease (MI, stroke) at entry to this study. Furthermore, benefits were also seen in the group of 2426 of these participants whose pretreatment LDL-cholesterol level was below 3.0 mmol/L. In both groups the effects of statin treatment (40 mg simvastatin over an average of 4.6 years) was significant with P <0.0003 and <0.0007, respectively (Figure 2).
Critics of the cholesterol-lowering treatment in primary prevention such as the Therapeutics Initiative group[7] argue that (a) the absolute risk reduction—which was 1.4% in the ASCOT-LLA and 4.4% in the MRC/BHF study—is small, (b) there is no statistically significant effect on total mortality and (c) there is an increase in other serious adverse effects in individuals treated with statins. I disagree for the following reasons:
The data analysis was done on an “intent to treat” basis, that is, anyone in the assigned group was considered either 100% adhering to the drug or 100% adhering to the placebo. This is, in practice, not the case as “contamination” of the two groups is common: for example, in the ALLHAT Study[8] 30% of the placebo group took statin treatment and this resulted in only small LDL-cholesterol differences between the groups (and no significant benefit of the treatment). Furthermore, events occurring within days or weeks of treatment with the drug are counted, though it is extremely unlikely that the atherosclerotic lesion stabilization occurs so fast. Indeed, the event and survival curves of placebo and drug-treated groups continue to diverge as time goes on. And finally the effect, as has been reviewed many times (for a review see Genest and Pedersen[9]), depends on the magnitude of lipid lowering. With radical lipid changes up to 90% of events were prevented in HATS.[10] Thus it is fair to conclude, as does the Oxford epidemiology group,[2] that the benefits of treatment are underestimated.
It is true that there have been no statically significant decreases in total mortality (although WOSCOPS came close with P = 0.051), but the primary prevention trials were not designed to answer this question. In the ASCOT-LLA study the safety monitoring committee decided to stop the trial when it was apparent that there is a significant cardiovascular benefit and continuation under these circumstances would be unethical.
In none of the statin trials was there any significant increase in a specific category of serious adverse events (SAE)—these were random events. SAEs have never been used as a trial endpoint. They are meant to be used as a safety monitoring tool, not as study endpoints. One can also ask a question regarding this: is it the same SAE to have a stroke or to have acute tonsillitis?
Is there a place for statin treatment of patients at high risk for atherothrombotic events? In posing the question I am purposely avoiding the terms of primary and secondary prevention: your patients at high risk (for example those with diabetes or chronic kidney disease, familial hypercholesterolemia, or combination of major risk factors) will switch from one category to another within minutes of onset of their chest pain and quite a few will not live to qualify for “secondary” prevention. A wealth of epidemiological, pathological, genetic, and clinical trial evidence supports the use of statins for patients at high risk of atherothrombotic events.
It does not mean that we should not make every effort to support healthy lifestyles and consider non-pharmacological alternatives to cholesterol lowering, such as promising dietary[12] and exercise regimens.[13]
Competing interests
Over the last 5 years Dr Frohlich has received honoraria, fees for speaking engagements, consultancy fees, and research grant support from Pfizer Canada, Merck Frosst Canada, Astra Zeneca, Fournier Pharma, and Forbes Medi Tech.
References
1. Sever PS, Dahlof B, Poulter NR, et al. Prevention of coronary and stroke events with atorvastatin in hypertensive patients who have average or lower-than-average cholesterol concentrations, in the Anglo-Scandinavian Cardiac Outcomes Trial—Lipid Lowering Arm (ASCOT-LLA): A multicentre randomised controlled trial. Lancet 2003;361:1149-1158. PubMed Abstract Full Text
2. Collins R, Armitage J, Parish S, et al. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: A randomised placebo-controlled trial. Lancet 2003;361:2005-2016. PubMed Abstract Full Text
3. Drummond GA. ASCOT-LLA: Questions about the benefits of atorvastatin. Lancet 2003;361:1987-1988. PubMed Citation Full Text
4. Hackam DG. Do hypertensive patients with average cholesterol levels benefit from atorvastatin therapy? CMAJ 2003;168:1689. PubMed Citation Full Text
5. Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk of vascular disease (PROSPER): A randomised controlled trial. Lancet 2002;360:1623-1630. PubMed Abstract Full Text
6. Collins R, Armitage J, Parish S, et al. MRC/BHF Heart Protection Study. Lancet 2002;360:1783-1784. PubMed Citation Full Text
7. Therapeutics Initiative. Therapeutics Letter # 48 April-May-June 2003. Vancouver: University of British Columbia. Full Text
8. ALLHAT Collaborative Research Group. Major outcomes in moderately hypercholesterolemic, hypertensive patients randomized to pravastatin vs usual care: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT-LLT). JAMA 2002;288:2998-3007. PubMed Abstract Full Text
9. Genest J, Pedersen TR. Prevention of cardiovascular ischemic events: High-risk and secondary prevention. Circulation 2003;107:2059-2065. PubMed Citation Full Text
10. Brown BG, Zhao XQ, Chait A, et al. Simvastatin and niacin, antioxidant vitamins, or the combination for the prevention of coronary disease. N Engl J Med 2001;345:1583-1592. PubMed Abstract Full Text
11. Shepherd J, Cobbe SM, Ford I, et al. Prevention of coronary heart disease with pravastatin in men with hypercholesterolemia. West of Scotland Coronary Prevention Study Group. N Engl J Med 1995;333:1301-1307. PubMed Abstract Full Text
12. Jenkins DJ, Kendall CW, Marchie A, et al. Effects of a dietary portfolio of cholesterol-lowering foods vs lovastatin on serum lipids and C-reactive protein. JAMA 2003;290:502-510. PubMed Abstract Full Text
13. Thompson PD, Buchner D, Pina IL, et al. Exercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: A statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity). Circulation 2003;107:3109-3116. PubMed Citation Full Text
Jiri Frohlich, MD, FRCPC
Dr Frohlich is a professor in the Department of Pathology and Laboratory Medicine at the University of British Columbia and academic director at St. Paul’s Hospital Healthy Heart Program/Lipid Clinic.

{kind=link}
{kind=link}