Evaluation of genetic counseling for hereditary cancer by videoconference in British Columbia
Issue: BCMJ,
vol. 50 , No. 10 , December 2008 ,
Pages 554-559 Clinical Articles
Background: Hereditary cancer accounts for up to 10% of the 5000 new cases of breast, ovarian, and colon cancer diagnosed in British Columbia each year. Many patients living in rural and remote areas of the province do not have easy access to the genetic counseling services provided in urban tertiary care centres. A study was designed to assess the acceptability and effectiveness of videoconferencing to deliver genetic counseling services to these patients.
Methods: Videoconference clinics were established to allow contact between the Hereditary Cancer Program in Vancouver and six rural hospitals as far as 1500 km away. Following each genetic counseling session, patients and counselors completed standardized satisfaction questionnaires based on a 5-point Likert scale. Data were collected from March 2005 to April 2006.
Results: Forty-three of 64 invited patients took part in the study, for a participation rate of 67%. The four counselors involved completed surveys for all of the sessions they participated in. Results from the patient and counselor surveys showed a favorable response to videoconference appointments. The patients benefited from saving considerable costs and time, and the majority preferred to receive counseling in their own communities. Some patients reported they would not have received counseling otherwise. When technical difficulties were experienced, they had a greater impact on counselor satisfaction than patient satisfaction.
Conclusions: Videoconferencing is an acceptable and effective means of providing hereditary cancer genetic counseling services. Most importantly, this technology can help patients living in rural and remote communities access specialty services.
Patients from rural and remote areas responded very favorably after taking part in telehealth consultations with genetic counselors based in Vancouver.
Approximately 14% of British Columbians live in rural and remote regions and have limited access to health services, including genetic counseling for hereditary cancer. The challenges posed by this situation promise to intensify with the rapid growth of new genetic technologies, the shortage of genetics professionals, and the economic necessity of providing specialty services in urban tertiary care centres.[1] Alternative approaches are needed to address the access barriers faced by rural citizens. This study aimed to evaluate the acceptability of providing genetic counseling by videoconference.
Hereditary cancer susceptibility syndromes account for 5% to 10% of the 5000 new cases of breast, ovarian, and colon cancers diagnosed in British Columbia each year. Currently, hereditary cancer services are provided by the provincial Hereditary Cancer Program (HCP), which is located in two urban tertiary care centres in Vancouver and Victoria. Even though outreach clinics are held in smaller centres periodically, families living in rural and remote areas of BC frequently do not receive the potential benefit of hereditary cancer genetic counseling services. Numerous studies have identified travel time, expense, and the need for time off work and child care as significant obstacles for rural patients referred to urban-based specialists and clinics.[2-5] Anecdotal evidence suggests that some rural physicians do not refer eligible patients to the HCP program because of the travel distance and associated costs involved (unpublished report by Horsman D, Kim-Sing C, Panabaker K, et al. Cancer Risk Assessment and Follow-up in BC Rural Communities: Needs Assessment and Educational Tools. Hereditary Cancer Program Report; 2002). Other reports also indicate that there is a great need for cancer-related information, services, and psychosocial support in northern and rural areas of the province.[6]
Genetic counseling for hereditary cancer is a clinical specialty that is well suited to delivery by videoconference. The primary focus of the genetics consultation is exchange of medical information and communication of related psychosocial issues. The sessions involve a detailed review of family history and medical records, a discussion of hereditary cancer biology and the likelihood that a hereditary cancer syndrome may be present, and a review of risk-management strategies based on the patient’s family history of cancer. When genetic testing is appropriate, genetic counseling also incorporates a detailed review of the pros and cons of having genetic testing, an explanation and interpretation of test results, and psychosocial support. Thus, genetic counseling is not limited by the need for high-resolution images or the rapid transfer of large-sized image files. The technology is quite able to accommodate graphics as an adjunct to verbal information.
In December 2002, the province of British Columbia completed a $6.5 million telehealth network development program. There are now over 70 BC communities with telehealth facilities, including regional centres, small hospitals, and community health clinics. Telehealth programs directed specifically at delivering genetic counseling for hereditary cancer have been successful in the UK[7],[8] Australia,[9] and the US.[10] To our knowledge, this is the first reported study using videoconferencing to provide genetic counseling for hereditary cancer in Canada.
Telehealth connections were made between the HCP in Vancouver and hospitals in six rural communities. Two members of the research team began by visiting these rural communities to talk to local health care providers about providing hereditary cancer education by videoconference. In addition to these site visits, a letter was sent to GPs, surgeons, and oncologists in these communities describing the study and inviting patient referrals. The first telehealth clinic was set up in August 2003 in a northern site located 800 km away from the HCP in Vancouver. Success with this pilot project led to the addition of three northern hospitals (at distances of 1500 km, 1260 km, and 1200 km) and two hospitals in the eastern region of the province (at distances of 628 km and 968 km) over the next 2 years.
Videoconference links were established in these clinics using either a Tandberg 6000 system (384 kbps ISDN transmission rate) or a Polycom VSX 7000s (384 kbps ISDN transmission rate via an Accord MGC 100 bridge). A document camera was also made available to transmit diagrams (e.g., family pedigree or illustrations) during the consultation.
Subjects
After ethics approval was obtained, potential study subjects were approached. Individuals were considered eligible for the study if they had been referred to the HCP because of a significant family history of cancer (e.g., breast, ovarian, colorectal cancer, and melanoma) and if they lived in the northern or eastern health regions of the province. Potential subjects were initially sent a letter about the project and a study consent form. Those who did not return the consent form were contacted by the project coordinator 6 weeks later, and asked whether they would like to participate in the study or to receive genetic counseling in person in Vancouver. Those who returned the completed consent form were contacted by a genetic counselor and asked for family information and other necessary medical records. A videoconferencing appointment was then booked and a letter was sent to the participant with directions to the videoconferencing site, name and contact information for the local telehealth coordinator, and information about what material to bring and what to expect at the appointment.
Data analysis
Patients (and family members, if they attended the consultation) were asked to complete a standardized satisfaction questionnaire immediately after their videoconferencing appointment. Participants used a 5-point Likert scale (from 1=strongly disagree to 5=strongly agree) to comment on a number of outcome variables, including comfort level, general satisfaction, comprehension of information, quality of service (simplicity, ease of use, technical difficulties), and estimated time and cost-savings for the subject. These measures have been established in other studies assessing the acceptability of videoconferencing for provision of genetic testing and oncology services.[8],[11],[12] Genetic counselors were also asked to complete a satisfaction questionnaire based on a 5-point Likert scale that was adapted from evaluation surveys used in other studies.[12] Data were collected from March 2005 to April 2006 and analyzed using descriptive statistics (e.g., frequencies, percentages, ranges, and mean).
Sixty-four patients were eligible to participate in the study. Of these, 43 (67%) agreed to participate and 21 declined. Of those who declined, 10 preferred a face-to-face consultation in Vancouver and 11 declined a genetic counseling appointment altogether. In addition to the 43 patients who participated, 5 family members participated, for a total of 48 responses. Counseling was provided by four genetic counselors from the HCP, who completed a questionnaire after each counseling session.
Patient responses
The results of the patient surveys summarized in [Table 1] show a high degree of satisfaction with the videoconference appointment (average 4.68 out of 5). Items assessing participants’ perceptions of the videoconferencing technology (questions 8, 9, 10) indicate that patients readily adapted to this format. For the most part, patients felt that they could communicate effectively, ask questions, and understand the information conveyed by the genetic counselor during the appointment. No participants reported that the video-based communication made it difficult for them to understand the information.
Major advantages reported included cost-savings (averaging $1000 per person); convenience (eliminated burden of travel or need to miss work); and ability to have family members present at the appointment. For the most part, patients preferred to be seen in their home communities and some reported they would not otherwise have followed through with their HCP referrals.
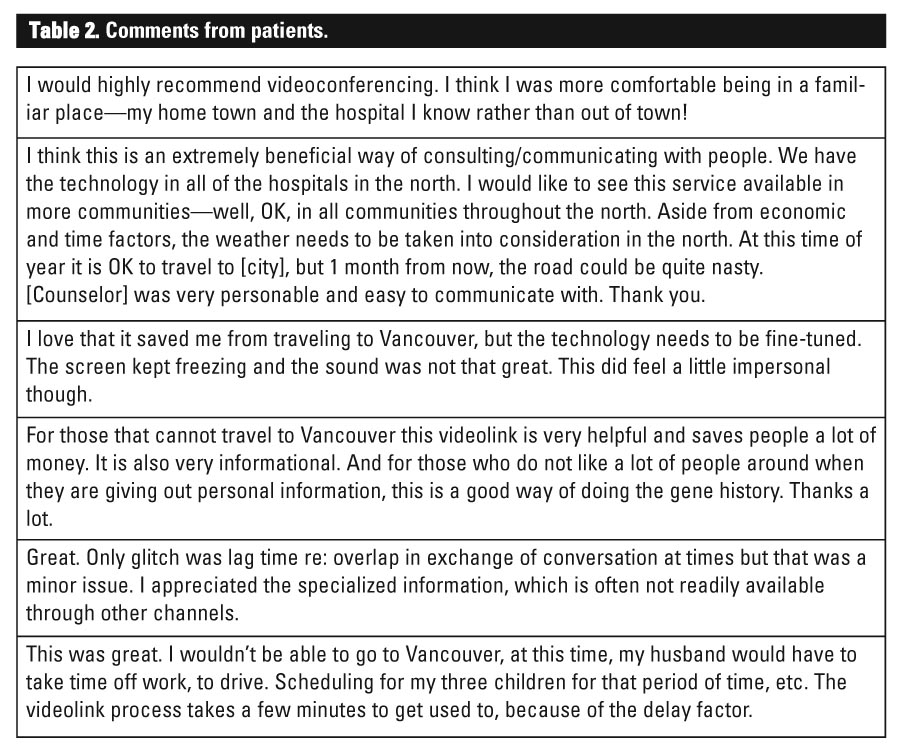
Responses to an open-ended request for comments also demonstrated support for the videoconferencing appointments [Table 2]. Patients valued the information obtained through the counseling process and they generally felt they were able to establish a personal connection with their genetic counselor. Again, convenience and cost-savings were cited as major advantages of the technology.
When technical difficulties (poor image or sound quality and loss of connection) did occur, they were the primary obstacle to satisfaction. A common drawback was the delay in audio transmission resulting in individuals speaking over one another. However, patients generally viewed these problems as minor and/or annoying rather than disruptive.
Genetic counselor responses
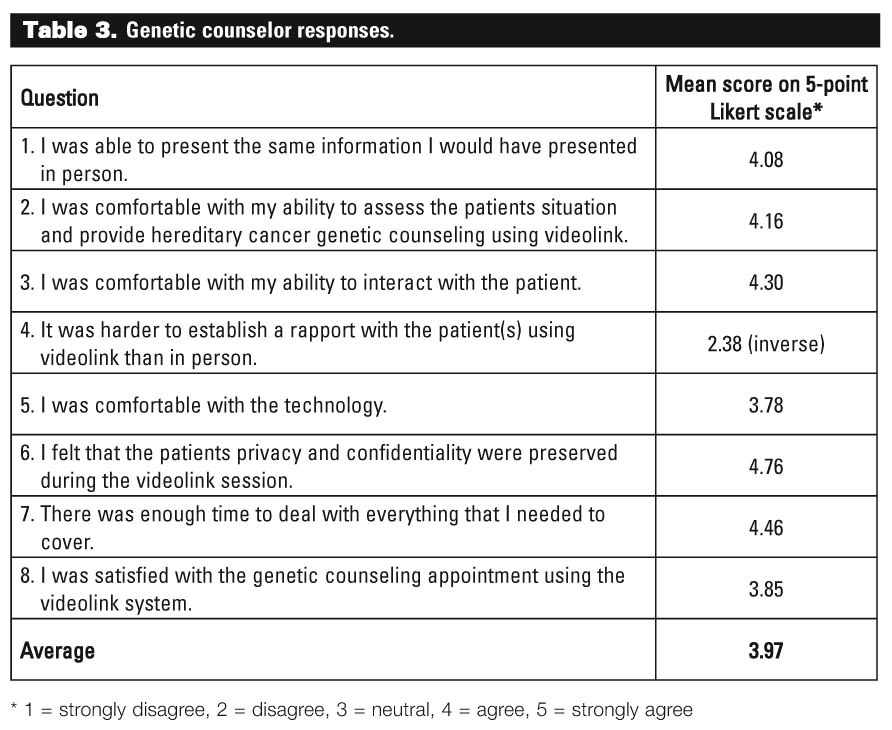
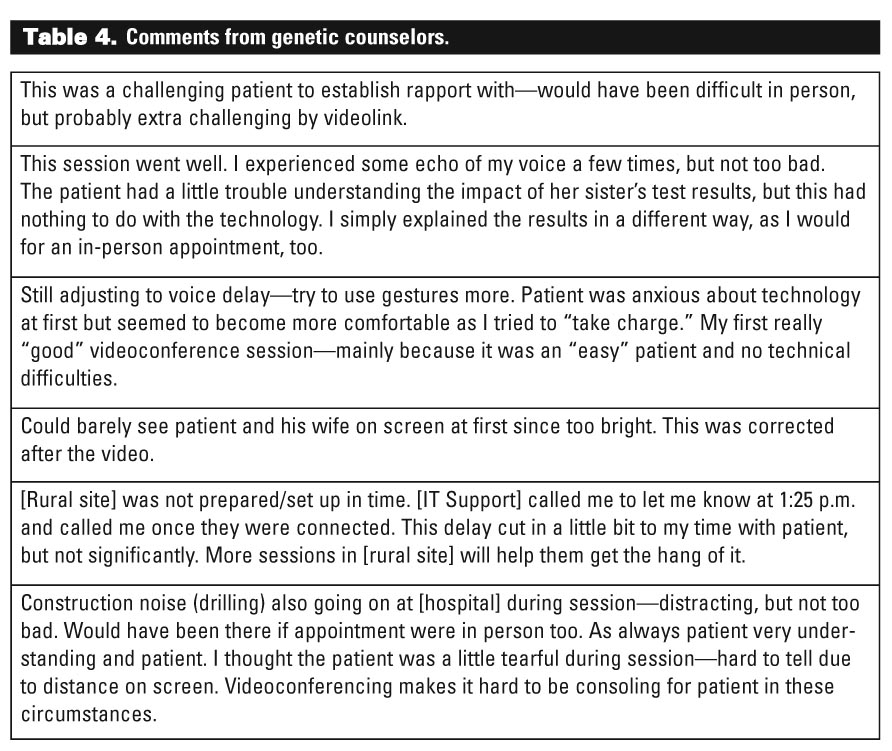
The results of the counselor satisfaction surveys shown in [Table 3] indicate that genetic counselors were less satisfied with the videoconference consultation than patients, although they were still highly satisfied (average 3.97 out of 5). Counselors found that the videoconferencing component added a new dimension of complexity to the appointment, and that the degree of rapport established with the patient influenced their level of satisfaction [Table 4].
Interestingly, genetic counselors’ perceptions of the videoconferencing appointment did not always match the patients’ reactions to the same event. Often, the genetic counselor was far more critical of minor disturbances that occurred during the session than the patient was, as the following responses indicate.
Genetic counselor: “During the session there were numerous sound interruptions due to construction nearby and announcements over the PA system. Hard to avoid/control, but annoying just the same.”
Patient: “Occasionally I was somewhat distracted by noises in the hallway and ongoing construction in the building. I think this is a valuable tool, especially for those who cannot afford time and cost of travel. Thank you for doing this.”
The difference in satisfaction rating between the counselors and patients may also be explained by differences in the valuation of different aspects of care.[13] As the following excerpt from the same session indicates, patients may value the access provided by videoconferencing so much that they are less concerned than the genetic counselors with slight reductions in communication quality.
Genetic counselor: “I find that my video sessions do not go into as much depth. I only give the basic necessary information and psychosocial issues do not get addressed in the same way as they do in person.”
Patient: “I was very satisfied with the videolink. It was a wintry day on my meeting and I would not have wanted to travel to Vancouver on icy roads, rearrange my work schedule, and leave my wife alone with our newborn. It was private and the sound and video were clear. The counselor was informative and thorough. Very positive way for me to accomplish this meeting.”
There were no cases where a patient expressed dissatisfaction with the counseling session and the genetic counselor expressed satisfaction.
In keeping with findings from other countries,[6-8],[10] the results of this BC study indicate that videoconferencing is an effective means of providing genetic counseling to rural and underserved populations. All patients who received genetic counseling by videoconference reported positive experiences with the technology. Videoconferencing was convenient, required little time off work, eliminated the need to travel great distances, and resulted in considerable cost-savings. Most importantly, it provided access to genetic consultations for some people whose economic or personal situation would have otherwise prevented access. Genetic counselors also reported satisfaction with the service, although to a lesser extent than patients, in accord with other studies assessing health care provider satisfaction.[8],[13]
There were limitations to this study. Patients were given a choice of videoconference or in-person appointments, and those who may have responded less positively to videoconferencing likely chose a face-to-face appointment instead and were not part of the study group. However, it is likely that this selection bias will reflect the group of patients who ultimately choose to receive genetic counseling by videoconference.
Overall, the findings demonstrate the potential of telehealth to address barriers to genetic counseling faced by rural patients. In addition to benefiting patients, videoconferencing offers cost advantages compared with outreach programs. For example, the travel costs for one genetic counselor to provide outreach care for 12 patients at a 2-day clinic in Kelowna amounts to $700. The cost of conducting the same number of counseling appointments by videoconference is nil because equipment has been previously purchased through operational funds. The savings are clearly greater for sites further away, especially when the small numbers of patients do not warrant the expense of holding an outreach clinic.
Videoconferencing is not meant to replace face-to-face services but to expand existing approaches to care. In any event, there are some limitations to videoconferencing. It is difficult to fit multiple family members on a screen and thus only a few family members (up to three) can take part in a consultation. Ad hoc or unplanned consultations are also a challenge. In addition, a telehealth program can only succeed if there is a strong alliance with a local champion. A support person is needed to assist patients at the remote site and act as a liaison between the remote site and the delivery site (in this case, the BCCA).[14],[15] In our experience, the remote site requires committed and enthusiastic service providers who must sometimes go beyond their usual job descriptions to assist with the practical arrangements. Communities where staff turnover is high—a common problem in many rural settings—will require ongoing training support from the tertiary care centre.[16]
As well as providing evidence that videoconferencing can be used to deliver care when geographic distances pose a barrier, these study findings may apply to other health service and clinical areas outside of genetic counseling, such as follow-up oncology,[11] orthopaedic or clinical genetics,[10] palliative care,[14] specialty mental health services, and psychiatric consultations.[13],[17],[18]
We would like to thank the women and men from hereditary cancer families who participated in this study. We would also like to acknowledge and thank the following individuals, without whose assistance the project could never have been completed: Helen Truran, Judith Rea, Deborah Polding, Val Paolini, and Susan Vlanich. This research was funded by a grant from the BC Medical Services Foundation. Dr d’Agincourt-Canning was supported by a postdoctoral training fellowship from the Canadian Institutes of Health during the study.
None declared.
References
1. Mitchell JA, Demiris G. Telegenetics: The next phase in the provision of genetics services? Genet Med 2005;7:1-2.
2. Kirby M, LeBreton M. The Health of Canadians—The Federal Role. Current Trends and Future Challenges. Vol 2. Ottawa, ON: Standing Committee on Social Affairs, Science and Technology, Parliament of Canada; 2002.
3. Jong KE, Vale PJ, Armstrong BK. Rural inequalities in cancer care and outcome. Med J Aust 2005;182:13-14.
4. Crosata KE, Leipert B. Rural women caregivers in Canada. Rural Remote Health 2006;6:520-531.
5. Sutherns R, McPhedran M, Hayworth-Brockman M. Rural, Remote and Northern Women’s Health: Policy and Research Directions. Final Summary Report. Winnipeg, MB: Centres of Excellence for Women’s health; 2003. www.cewh-cesf.ca/PDF/cross_cex/RRN_Summary_CompleteE.pdf (accessed 30 September 2008).
6. BC Cancer Agency and Northern Health. Northern Cancer Control Strategy Final Report. Vancouver, BC: BCCA; 2005. Click to view (accessed 30 September 2008).
7. Coelho JJ, Arnold A, Nayler J, et al. An assessment of the efficacy of cancer genetic counselling using real-time videoconferencing technology (telemedicine) compared to face-to-face consultations. Eur J Cancer 2005;41:2257-2261.
8. Gray J, Brain K, Iredale R, et al. A pilot study of telegenetics. J Telemed Telecare 2000;6:245-247.
9. Gattas MR, MacMillan JC, Meinecke I, et al. Telemedicine and clinical genetics: Establishing a successful service. J Telemed Telecare 2001;7(suppl2):68-70.
10. Lea DH, Johnson JL, Ellingwood S, et al. Telegenetics in Maine: Successful clinical and educational service delivery model developed from a 3-year pilot project. Genet Med 2005;7:21-27.
11. Weinerman B, den Duyf J, Hughes A, et al. Can subspecialty cancer consultations be delivered to communities using modern technology? A pilot study. Telemed J E Health 2005;11:608-615.
12. Centre for Telehealth @Mheccu. Telehealth Handbook. Vancouver: Mental Health Evaluation and Community Consultation Unit; 2003. www.carmha.ca/publications/resources/pub_ctmthb/Telehealth%20Handbook.pdf (accessed 30 September 2008).
13. Cruz M, Krupinski EA, Lopez AM, et al. A review of the first five years of the University of Arizona telepsychiatry programme. J Telemed Telecare 2005;11:234-239.
14. MacFarlane A, Murphy AW, Clerkin P. Telemedicine services in the Republic of Ireland: An evolving policy context. Health Policy 2006;76:245-248.
15. Brebner JA, Brebner EM, Ruddick-Bracken H. Experience-based guidelines for the implementation of telemedicine services. J Telemed Telecare 2005;11(suppl1):3-5.
16. Watson J, Gasser L, Blignault I, et al. Taking telehealth to the bush: Lessons from North Queensland. J Telemed Telecare 2001;7(suppl2):20-23.
17. Brasfield C, Clement C. Beyond the pilot studies: Cognitive behavioural therapy in a remote aboriginal community. Presented at the10th Annual Conference of the Canadian Society of Telehealth, St. John’s, NL, 4-6 November 2007. www.nssac.ca/Resources.htm (accessed 30 September 2008).
18. Urness D, Hailey D, Delday L, et al. The status of telepsychiatry services in Canada: A national survey. J Telemed Telecare 2004;10:160-164.
Dr d’Agincourt-Canning is a clinical assistant professor in the Department of Pediatrics at the University of British Columbia, and co-director of the Clinical Ethics Service, BC Children’s and Women’s Health Centre. Dr McGillivray is a professor in the Department of Medical Genetics at UBC, and a clinical geneticist with the Provincial Medical Genetics Program, BC Children’s Hospital, and the Hereditary Cancer Program, BC Cancer Agency (BCCA). Ms Panabaker is a genetic counselor at the London Regional Cancer Program in London, Ontario. Ms Scott is head genetic counselor for the Hereditary Cancer Program, BCCA, and clinical instructor in the Department of Medical Genetics, UBC. Ms Pearn is a genetic counselor with the Division of Medical Genetics at Royal University Hospital in Saskatoon, Saskatchewan. Ms Ridge is a genetic counselor and clinical assistant professor in the Department of Medical Genetics, UBC. Ms Portigal-Todd is a genetic counselor with the Hereditary Cancer Program, BCCA, and clinical instructor in the Department of Medical Genetics, UBC.

{kind=link}
{kind=link}
{kind=link}