Coronary computed tomographic angiography in British Columbia: A review
Issue: BCMJ,
vol. 49 , No. 2 , March 2007 ,
Pages 78-84 Clinical Articles
Coronary computed tomographic angiography utilizing multidetector technology allows for the noninvasive detection and quantitation of coronary artery disease at a significantly higher level of safety and at a lower cost than catheter coronary angiography. In addition, this imaging modality provides information about cardiac structure and function. Appropriate patient selection is crucial to the optimal use of this technology.
Certain patients may benefit from a noninvasive imaging technique that detects coronary artery disease and provides information about cardiac structure and function.
Coronary computed tomographic angiography (CCTA) is performed by injecting an intravenous contrast agent and then imaging the heart during a single breath hold utilizing multidetector (MDCT) technology. This new clinical tool allows for the noninvasive detection and quantitation of coronary artery disease (CAD) at a significantly higher level of safety and at a lower cost than conventional invasive coronary angiography. In addition, CCTA provides information related to cardiac structure and function.
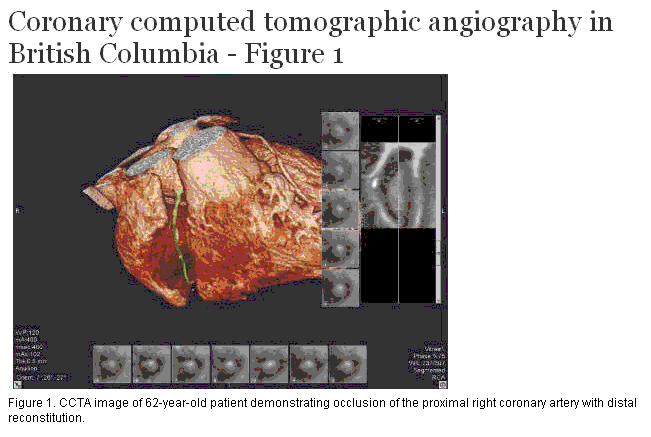
A 62-year-old dyslipidemic man with no previously documented coronary artery disease presented with a 2-year history of atypical chest pain that had increased in frequency and severity for the preceding 3 months. Echocardiography as well as an exercise myocardial perfusion study (MIBI stress test) were reported as normal, with an exercise time of 8 minutes using the Bruce protocol. The patient was taking ASA and trazodone at the time of presentation. Further clinical examination revealed no other pertinent information.
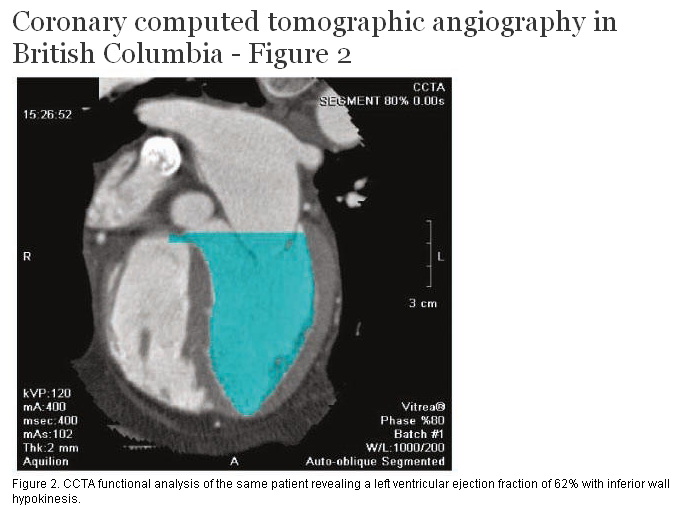
CCTA (Figure 1) revealed the proximal right coronary artery to be occluded, with distal reconstitution of the vessel. The left-sided circulation demonstrated moderate atherosclerotic plaque burden but no flow-limiting stenoses. There was inferior wall hypokinesis; however, the left ventricular ejection fraction and left ventricular mass were normal (Figure 2). The ejection fraction and hypokinesis were assessed on the basis of a looping video image of the heart at multiple phases of the cardiac cycle, which allowed for assessment of wall motion.
{kind=link}
{kind=link}
Drug therapy, consisting of a beta-blocker, angiotensin converting enzyme inhibitor, and a statin, was introduced. The patient was then referred for catheter coronary angiography (Figure 3). This confirmed the presence of an occluded right coronary artery, which was successfully treated with angioplasty and stenting. The patient’s chest pain subsequently resolved.
{kind=link}
CCTA can be performed on units with 16 or more detector rows. However, recent studies have demonstrated significantly improved sensitivity and specificity for lesion detection when 64-detector technology (64-CT) is utilized.[1-4] Close to 100% of coronary arteries greater than 1.5 to 2.0 mm in diameter are reportedly assessable with 64-CT, whereas studies with 16-CT report only 70% of similar vessels are assessable.[5]
The rapid acquisition time required to successfully image the small, tortuous coronary arteries without motion artifact relates to the speed at which the bank of detectors (gantry) rotate around the patient. Gantry rotation time for 64-CT scanners is typically 330 to 400 ms, compared with 400 to 500 ms for 16-CT. The greater number of detectors with 64-slice technology results in improved spatial resolution, equaling 0.4-mm slice thickness.
CCTA typically involves intravenous injection of 90 mL of an iodinated contrast agent followed immediately by a saline flush. This volume is similar to that required for diagnostic coronary angiography. Imaging is performed during a single breath hold, with a study acquisition time of approximately 10 seconds for 64-CT and approximately 30 seconds for 16-CT.
Because image quality improves with lower heart rates, beta-blockers are often utilized in individuals with heart rates above 65 beats per minute. Sublingual nitroglycerin is given immediately before the exam because of its coronary vasodilatory effect.
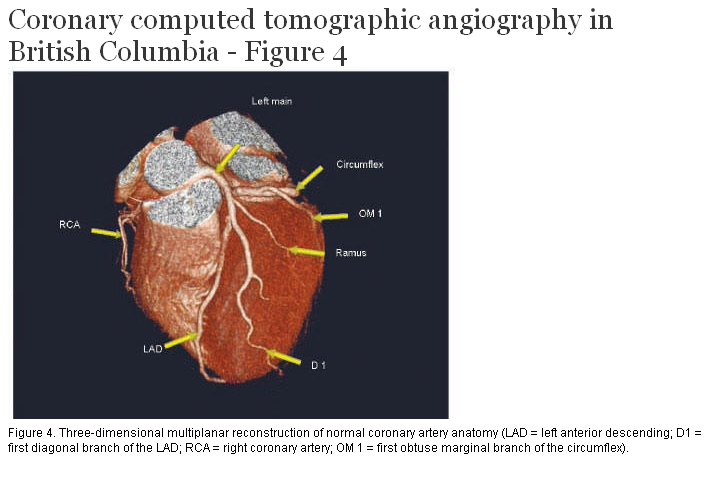
The acquired images are viewed directly and also reconstructed in multiplanar two- and three-dimensional formats for coronary artery assessment (Figure 4). Unlike catheter angiography, which is basically a “luminogram,” CT angiography potentially allows for the characterization of plaque composition, including positive remodeling and necrotic lipid core, two factors associated with plaque instability. While CCTA is not able to reliably and consistently diagnose plaque as “vulnerable” or unstable, it does permit additional analysis that can evaluate ventricular function and determine left ventricular mass. The visualized noncardiac anatomy can be evaluated for pathology, with common findings including pulmonary nodules, hiatal hernias, and focal liver lesions. Of note, approximately 16% of individuals are found to have significant noncardiac findings.[6]
{kind=link}
The utility of CCTA in an emergent setting is currently being evaluated in the hope that it can be used to rule out an acute coronary syndrome, aortic dissection, or pulmonary embolism in individuals with atypical presentations. Recently, a number of hospitals in the Lower Mainland and Victoria have started performing CCTA with 64-CT scanners. Canada Diagnostic Centres in Vancouver is the only private facility in British Columbia currently performing 64-CT. More than 250 patients have had CCTA performed at the centres so far.
Technical limitations and risks
CCTA is technically limited in patients who have a fast or irregular heart rate (owing to motion artifact). It is also limited in patients with extensive coronary calcification, which limits visualization of the lumen, and in very obese subjects, whose obesity degrades image quality.
CCTA requires a radiation dose in the range of 8 to 15 milliSieverts.[7] Other frames of reference include coronary artery calcification scoring (1.3 mSv), routine abdominopelvic CT imaging (10 mSv), myocardial perfusion imaging (8 mSv for technecium-99m and 18 mSv for thallium-201), invasive coronary artery angiography (6 mSv),[7] and average annual background radiation (2 mSv in Vancouver).
The use of an intravenous contrast agent is associated with a small risk of anaphylactoid reaction and nephropathy. Discomfort or bruising at the vein injection site (usually the forearm or hand) may also occur.
The most common indications for CCTA are:
• Atypical chest pain.
• Equivocal or inconclusive noninvasive cardiac testing.
• Interval assessment of documented coronary artery disease.
• Assessment of coronary artery stents and bypass grafts.
• Unexplained left ventricular systolic dysfunction.
• Preoperative assessment of valvular heart disease.
• Multiple strong risk factors but no previously documented coronary artery disease.
The contraindications for CCTA are:
• Extensive coronary artery calcification (e.g., Agatston score > 1500).
• Chronic renal disease of sufficient severity to prohibit use of intravenous contrast agents (calculated GFR < 30).
• Irregular or rapid heart rates (e.g., atrial fibrillation or frequent ventricular or supraventricular ectopy).
• Allergy to intravenous contrast agents.
• Inability to hold breath or remain motionless for 10 seconds.
• High likelihood of requiring percutaneous coronary intervention.
Correlation with invasive coronary angiography
Raff and colleagues studied 70 consecutive patients who underwent both 64-CCTA and invasive coronary angiography.[1] In 935 of 1065 segments (88%), high correlation was observed, with a Spearman correlation coefficient of 0.76 (P<.0001). The CCTA results were assessed for sensitivity (sn), specificity (sp), positive predictive value (ppv), and negative predictive value (npv). By artery (N = 279), there was sn of 91%, sp of 92%, ppv of 80%, and npv of 97%. By patient (N = 70), there was sn of 95%, sp of 90%, ppv of 93%, and npv of 93%. A greater than 50% narrowing was defined as a significant stenosis in this study.
Mollet and colleagues performed CCTA on 52 patients scheduled for invasive coronary angiography because of atypical chest pain, stable or unstable angina, or non-ST-elevation myocardial infarction.[2] The values for sn, sp, ppv, and npv for stenoses greater than 50% were 99%, 95%, 76%, and 99%, respectively.
Gaspar and colleagues observed CCTA using a 40 MDCT unit to examine 65 patients with 111 stents referred for repeat invasive coronary angiography.[8] They reported sn of 72.2%, sp of 92.5%, ppv of 65.0%, and npv of 94.5% in the assessment of in-stent restenosis of greater than 50%. The clinical utility of CCTA for the detection of in-stent restenosis was noted to be probably best suited to patients with a low clinical suspicion.
Correlation with intravascular ultrasound
Leber and colleagues studied the diagnostic accuracy of 64-CCTA in 59 patients undergoing invasive coronary angiography for angina.[3] Intravascular ultrasound (IVUS) was performed in 32 vessels. They reported sensitivities for detection of coronary artery stenoses less than 50%, greater than 50%, and greater than 75% were 79%, 73%, and 80%, respectively, with a specificity of 97%. An excellent correlation existed between the two techniques in the measurement of plaque cross-sectional area.
Van Mieghem and colleagues studied the correlation between IVUS and CCTA in 67 patients, defining a significant stenosis as greater than 50% of the luminal diameter.[9] Compared with IVUS, CCTA had sn of 86%, sp of 69%, ppv of 90%, and npv of 61%.
Correlation with cardiac magnetic resonance imaging
Mahnken and colleagues compared 16-detector row contrast CT with contrast-enhanced cardiac magnetic resonance (CCMR) imaging in 28 patients within 2 weeks of an acute myocardial infarction.[10] The authors concluded that late-enhancement contrast CT seems to be as reliable as delayed CCMR for assessing infarct size and myocardial viability following acute myocardial infarction.
Several studies have compared left ventricular (LV) ejection fraction measurements using CCTA and MRI, and have reported an excellent correlation (r = 0.83 to 0.89) between the two modalities.[11-16] LV end-diastolic and end-systolic volumes have also correlated well (r = 0.80 to 0.93, and r = 0.89 to 0.94, respectively).
MRI is still limited in its ability to visualize coronary anatomy owing to technical difficulties in dealing with motion artifact. However, MRI has the advantage of no ionizing radiation exposure for the assessment of viability and visualization of noncoronary anatomy.[11-16]
Correlation with transthoracic echocardiography
Feuchtner and colleagues evaluated the diagnostic accuracy of 16-detector CCTA in patients with aortic stenosis.[17] When compared with transthoracic echocardiography (TTE), the sensitivity of CCTA for the identification of aortic stenosis was 100%, with a specificity of 93.7%. Quantification of aortic valve area with CCTA showed a good correlation with TTE (r = 0.89, P <.001). The role of CCTA in valvular assessment is still being clarified.
The role of coronary artery calcium scoring
Coronary artery calcium (CAC) scoring, which is done routinely at the time of CCTA, was discussed in a recent review by Forster and Isserow.[18] Whether a patient should undergo CAC screening instead of CCTA can be determined by considering risk factors and symptoms (Figure 5).
{kind=link}
Elevated Agatston scores (>400) add independent prognostic information to the traditional risk factors in individuals with an intermediate Framingham risk score. A recent study of 1983 lower-risk patients (with a mean 10-year Framingham risk score of 4.6% for men and 1.4% for women) demonstrated that screening for the presence of coronary artery calcification has cost-effective, independent prognostic value in predicting incident coronary heart disease risk that is incremental to conventional coronary risk factors.[19]
A very low Agatston score (<10) in individuals at low risk of having coronary atherosclerosis may be used to justify not proceeding with CCTA and exposing the patient to the contrast agent and excess radiation, although this strategy has not been validated clinically. A limitation of this approach is that a small percentage of individuals may have significant stenoses related to noncalcified atherosclerotic plaque despite a low CAC score. This situation is most often seen in young male smokers. Conversely, a very high Agatston score (>1500) is usually associated with extensive and significant coronary artery disease, and proceeding with CCTA in these patients usually does not change clinical management, as these patients require aggressive secondary prevention therapy as well as invasive coronary angiography, assuming they are candidates for revascularization.
CCTA is an emerging noninvasive imaging modality for the noninvasive identification and characterization of coronary artery atherosclerosis. In addition, the examination provides information regarding cardiac structure and function, and permits visualization of noncardiac anatomy. Significant noncardiac findings are sometimes demonstrated.
Preliminary studies are evaluating the utility of CCTA in the assessment of patients presenting to the emergency room with chest pain. With the increasing availability of CCTA, it is likely that this technology will be far more widely used in the near future.
Dr Heilbron receives a fee for interpreting coronary CT angiograms at the Canada Diagnostic Centres in Vancouver, BC. He has no ownership or other financial interest in Canada Diagnostic Centres.
| Frequently asked questions about coronary computed tomographic angiography
Is CCTA just an investigational tool or is it useful clinically? In selected patients, CCTA provides an accurate and clinically relevant assessment of coronary artery atherosclerosis, wall motion, ventricular systolic function, and cardiac mass. This technology is currently being used clinically in British Columbia, but accessibility has been limited by the absence of a reimbursement code in Canada or the US. Patients should be scanned in centres that have 64-slice CT technology and staff specifically trained in CCTA acquisition and interpretation. Who should not have CCTA? Patients with the contraindications listed here, and patients who have a high pretest probability of requiring revascularization should not have CCTA. In patients with a very low pretest probability of having coronary atherosclerosis, the risks and cost of the test should be weighed against the very low likelihood of the test changing clinical management. What is the cost? The cost of CCTA at Canada Diagnostic Centres is $2200. The examination does not yet have a Medical Services Plan of British Columbia fee code. Although a number of British Columbia public hospitals are starting to perform the examination, it is not yet being offered routinely. Is CCTA as good as invasive coronary angiography for the assessment of the presence or severity of coronary artery disease? The sensitivity and specificity of CCTA versus invasive coronary angiography for the detection and quantitation of coronary atherosclerosis in selected patients is greater than 95%.[20] The temporal resolution of CCTA is not quite as good as invasive coronary angiography (as low as 100 to 200 ms using multidetector scanning versus 15 to 30 ms for invasive coronary angiography), but is sufficient to make a clinical diagnosis and plan appropriate therapy in the majority of patients. How long does the procedure take? The actual study is performed within a single breath hold. The entire procedure (including patient preparation) takes approximately 1 hour. What are the risks associated with invasive coronary angiography? The risks of bruising at the access site are generally noted as being less than 25%, and the risks of major complications such as myocardial infarction, stroke, death, damage to a major vessel, need for dialysis, or infection are less than 2% combined.[21] What is the role of coronary artery calcium screening now that CCTA is available? Coronary artery calcium screening provides an assessment of the risk of coronary atherosclerosis, which can be considered along with the Framingham risk score. It is a less expensive test (approximately $700) than CCTA and involves less radiation exposure (approximately 1.3 mSv) with no intravenous contrast administration.[22] However, the Agatston score is a surrogate marker for atherosclerosis, and occasionally individuals with significant noncalcified atherosclerotic plaque can have a low Agatston score. |
References
1. Raff GL, Gallagher MJ, O’Neill W, et al. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol 2005;46:552-557. PubMed Abstract Full Text
2. Mollett NR, Cademartiri F, Nieman K, et al. Multislice spiral computed tomography coronary angiography in patients with stable angina pectoris. J Am Coll Cardiol 2004;43:2265-2270. PubMed Abstract Full Text
3. Leber A, Knez A, Ziegler F, et al. Quantification of obstructive and nonobstructive coronary lesions of 64-slice computed tomography: A comparative study with quantitative coronary angiography and intravascular ultrasound. J Am Coll Cardiol 2005;46:147-154. PubMed Abstract Full Text
4. Leschka S, Alkhadi H, Plass A, et al. Accuracy of MSCT coronary angiography with 64-slice technology: First experience. Eur Heart J 2005;26:1482-1487. Full Text
5. Hoffmann MH, Shi H, Schmitz BL, et al. Noninvasive coronary angiography with multislice computed tomography. JAMA 2005;293:2471-2478. PubMed Abstract Full Text
6. Juergens KU, Grude M, Maintz D, et al. Multi-detector-row CT of left ventricular function with dedicated analysis software versus MR imaging: Initial experience. Radiology 2004;230:403-410. Full Text
7. Coles D, Smail M, Negus I, et al. Comparison of radiation doses from multislice computed tomography coronary angiography and conventional diagnostic angiography. J Am Coll Cardiol 47;9:1840-1848. PubMed Abstract Full Text
8. Gaspar T, Halon DA, Lewis BS, et al. Diagnosis of coronary in-stent restenosis with multidetector row spiral computed tomography. J Am Coll Cardiol 2005;46:1573-1579. PubMed Abstract Full Text
9. Van Mieghem CA, McFadden E, de Feyter PJ, et al. Noninvasive detection of subclinical coronary atherosclerosis coupled with assessment of changes in plaque characteristics using novel noninvasive imaging modalities: The Integrated Biomarker and Imaging Study (IBIS).. J Am Coll Cardiol 2006;47:1134-1142. PubMed Abstract Full Text
10. Mahnken AH, Gunther RW, Krombach GA. The basics of left ventricular functional analysis with MRI and MSCT. Rofo 2004;176:1365-1379. PubMed Abstract Full Text
11. Manning WJ, Li W, Edelman RR. A preliminary report comparing magnetic resonance coronary angiography with conventional angiography. N Engl J Med 1993;328:828. PubMed Abstract Full Text
12. Kim WY, Danias PG, Stuber M, et al. Coronary magnetic resonance angiography for the detection of coronary stenoses. N Engl J Med 2001;345:1863-1869. PubMed Abstract Full Text
13. Kefer J, Coche E, Legros G, et al. Head-to-head comparison of three-dimensional navigator-gated magnetic resonance imaging and 16-slice computed tomography to detect coronary artery stenosis in patients. J Am Coll Cardiol 2005;46:92-100. PubMed Abstract Full Text
14. Weiss JL, Shapiro EP, Buchalter MB, et al. Magnetic resonance imaging as a noninvasive standard for the quantitative evaluation of left ventricular mass, ischemia, and infarction. Ann N Y Acad Sci 1990;601:95-106. PubMed Abstract
15. Grude M, Juergens KU, Wichter T, et al. Evaluation of global left ventricular myocardial function with electrocardiogram-gated multidetector computed tomography: Comparison with magnetic resonance imaging. Invest Radiol 2003;38:653-661. Full Text
16. Halliburton SS, Petersilka M, Schvartzman PR, et al. Evaluation of left ventricular dysfunction using multiphasic reconstructions of coronary multi-slice computed tomography data in patients with chronic ischemic heart disease: Validation against cine magnetic resonance imaging. Int J Cardiovasc Imaging 2003;19:73-83. Full Text
17. Feuchtner GM, Dichtl W, Friedrich GJ, et al. Multislice computed tomography for the detection of patients with aortic stenosis and quantitation of severity. J Am Coll Cardiol 2006;47:1410-1417. PubMed Abstract Full Text
18. Forster BB, Isserow S. Coronary artery calcification and subclinical atherosclerosis: What’s the score? BCMJ 2005;47:181-187. PubMed Abstract Full Text
19. Taylor A, Bindeman J, Feuerstein A, et al. Coronary calcium independently predicts incident premature coronary heart disease over measured cardiovascular risk factors. Mean three-year outcomes in the prospective army coronary calcium (PACC) project. J Am Coll Cardiol 2005;46:807-814. Full Text
20. Achenbach S. Computed tomography coronary angiography. J Am Coll Cardiol 2006;48;1919-1928. PubMed Abstract Full Text
21. Baim DS, Grossman W. Complications of cardiac catheterization. In: Baim DS, Grossman W (eds). Cardiac Catheterization, Angiography and Intervention. Baltimore: Williams Wilkins; 1996:17.
22. Administration of Radioactive Substances Advisory Committee. Notes for guidance on the clinical administration of radiopharmaceuticals and use of sealed radioactive sources. Appendix I. www.arsac.org.uk/notes_for_guidence/docs/arsac_nfg.pdf (accessed 21 March 2006).
Brett Heilbron, MB ChB, FRCPC, FACC, Gordon Andrews, MD, FRCPC, Saul Isserow, MB BCh, FRCPC, FACC, Bruce B. Forster, MD, MSc, FRCPC
Dr Heilbron is a clinical assistant professor at the University of British Columbia and a member of the Division of Cardiology at St. Paul’s Hospital. His interests include noninvasive cardiac imaging and the early detection and treatment of coronary artery disease. Dr Andrews is an assistant professor of radiology at UBC and on active staff at UBC and Vancouver General Hospital. Dr Isserow is a clinical assistant professor at UBC and a staff cardiologist at UBC Hospital and Vancouver General Hospital. He is also director of the Vancouver General Hospital Centre for Cardiac Rehabilitation. Dr Forster is associate professor and vice-chairman (Research) of Radiology at UBC. He is also medical director of Canada Diagnostic Centres (BC). All authors co-interpret CCTA images at Canada Diagnostic Centres in Vancouver.