Coordination of radiological and clinical care for breast cancer diagnosis in BC
Issue: BCMJ,
vol. 60 , No. 1 , January February 2018 ,
Pages 33-39 Clinical Articles
ABSTRACT: The diagnosis of breast cancer has grown increasingly complex and delays can occur at multiple points in the clinical process. In 2010 the Provincial Breast Health Strategy was developed to optimize the clinical pathway for breast cancer diagnosis using a hub-and-spoke model for imaging and assessment. Each full-service diagnostic facility (hub) would provide imaging, anatomical pathology, surgical, and oncology services, while the Screening Mammography Program, family physicians, community imaging clinics, and hospitals (spokes) would refer women directly to the facility as needed. Hubs in each health authority would be required to meet the standard of care: core biopsy performed by a radiologist using image guidance and Breast Imaging Reporting and Data System (BI-RADS) classification and radiologic-pathologic correlation. The criteria for hubs would require having an accredited imaging department able to provide diagnostic ultrasound, wire localization, stereotactic biopsy, and other services using digital mammography equipment and related information systems. Hubs would also be expected to provide services according to available guidelines and protocols, and to collect information required to measure performance and audit practice. Another initiative to improve breast cancer diagnosis has been the development of coordinated care programs at Mount Saint Joseph Hospital and other institutions. Although these have been found to reduce wait times and be cost-effective, the lack of substantive permanent funding to support these programs has resulted in the loss of services at some centres and increasing wait times. To optimize patient experience and minimize wait times, we recommend province-wide acceptance and implementation of the Provincial Breast Health Strategy so that women navigating the diagnostic and therapeutic process receive coordinated care and support from a team of health care providers.
A hub-and-spoke model for facilities engaged in imaging and assessment for breast cancer diagnosis is needed to optimize patient experience and minimize wait times.
As breast cancer is the most common cancer in women, the need for more breast imaging, diagnostic, and treatment services will likely increase as the population grows and ages. There have been multiple attempts over the past 25 years to improve the diagnostic process for women in British Columbia who present with breast symptoms or have an abnormal screening mammogram and require further imaging, surgical consultation or care, and oncology services. Currently, the major initiative for improving breast cancer prevention, screening, and diagnosis in BC is the Provincial Breast Health Strategy (PBHS).[1]
Provincial Breast Health Strategy
In 2009 the Ministry of Health asked the Provincial Health Services Authority to devise a breast health action plan. This plan was completed in May 2010 and led to implementation of the Provincial Breast Health Strategy.[1] Objectives of the PBHS include developing a provincial clinical pathway that streamlines the process for women passing through the health care system by linking various diagnostic steps and centres, and using a hub-and-spoke model to improve the delivery of breast health services in the province.
After a review of provincial breast cancer screening policy was completed in 2011, a strategy to reduce the number of surgical biopsies and increase the number of image-guided biopsies was implemented with some success.[2] A business case was made for converting from analog to digital mammography, and a plan was developed to replace aging equipment. Cost-savings were obtained by using a provincial request for proposal and a single vendor. Once the last analog units are replaced in the Northern Health region, the province-wide conversion to digital mammography will be complete.
Following other PBHS recommendations, a number of radiologists have passed through the radiology fellowship training programs in breast imaging offered jointly by BC Women’s Hospital and BC Cancer, and cross-training programs for mammography and breast ultrasound technologists have resulted in the placement of a number of successful candidates around the province. In addition, partnerships with organizations such as the Canadian Breast Cancer Foundation and the Canadian Cancer Society have permitted online communication of evidence-based messages to women and physicians regarding prevention and screening.[3]
Health authority reports have been developed to provide HAs with important performance indicators, such as time from abnormal screen to diagnosis, and these continue to be shared to guide the evaluation process and promote shared accountability (written communication with Janette Sam, operations director, Screening Mammography Program of BC, 19 June 2017).
Before the years 2009 to 2012, when the provincial clinical pathway and hub-and-spoke model for breast diagnostic and surgical services were operative and had the most influence, some successful models of a breast centre existed. The most successful has been the Diagnostic Breast Program at Victoria General Hospital, which began in 1995. This centre has provided women with same-day diagnostic and biopsy services for over 20 years (written communication with Tammy Clark, supervisor, Breast Imaging, Victoria General Hospital, 20 June 2017), and has meant the South Island health service delivery area has the shortest time from screening to diagnosis in the province.4 Other examples of successful programs include the breast health clinic at the Jim Pattison Outpatient Unit in Surrey and the breast health clinic at the Abbotsford Regional Hospital and Cancer Centre.
Historically, breast imaging, diagnostic, and surgical services in the Vancouver area have been particularly fragmented. This has resulted from having a number of hospital-based facilities and community imaging clinics (CICs) play important roles in the delivery of services. Each community has a unique combination of facilities for breast diagnosis with varying degrees of integration between them. In Vancouver itself, breast imaging services are provided at BC Women’s, Mount Saint Joseph Hospital (MSJ), and BC Cancer. In addition, two large CICs, Xray 505 (headed by Dr Linda Warren) and Greig Associates, also perform diagnostic breast imaging services and image-guided biopsy, and host large breast screening clinics for the Screening Mammography Program (SMP). BC Women’s also has a smaller screening centre, as does MSJ. Other CICs provide diagnostic services using mammography and breast ultrasound.
MSJ, BC Women’s, and BC Cancer, as well as some of the CICs, carry out preoperative imaging for women requiring wire localizations prior to surgery. Breast cancer surgery is performed at MSJ and BC Cancer, as well as at Vancouver General Hospital (VGH) and the University of British Columbia Health Sciences Centre.
Women may have a localization procedure performed at one centre, such as BC Cancer, and then with the wire in situ have to transport themselves by driver or taxi to another centre, such as VGH, for their surgery. The challenges when coordinating all of this diagnostic work, as well as the surgical planning and treatment, are considerable. This fragmentation also leads to potential duplication of bookings and services, which is inefficient and costly to the system.
Northern Health has considerable challenges as well, although these are largely due to geography, small populations, and isolation. Women may have to travel long distances from home for their diagnostic tests and treatment and this often results in delays.[4]
Provincial clinical pathway
The provincial clinical pathway was developed to streamline the imaging, diagnostic, and surgical process, to prevent duplication, and to assist women and their family physicians as they progress through the system (Figure 1). The pathway was developed as part of the PBHS by a team of radiologists, surgeons, pathologists, medical and radiation oncologists, mammography technologists, administrators, and representatives of the Ministry of Health, with input from family physicians and other medical and oncology specialists as needed. The pathway timelines and standards were based on international guidelines and a number of very successful programs already operating in Europe.[5]
Implementation of the clinical pathway was facilitated by the introduction of a fast track referral policy by the Screening Mammography Program in 2010. This requires facilities to perform and report on diagnostic imaging procedures within 14 days of receiving the referral. Such fast track referrals permit a timely diagnostic journey and do not require the referring physician to orchestrate the process, although the physician is kept informed of the results and progress. The proposed time from abnormal screen or presentation with symptoms to the diagnostic result was set at 21 days.[6] Women receiving a cancer diagnosis are then to be seen by a multidisciplinary team of specialists, as needed, before beginning the therapeutic journey.
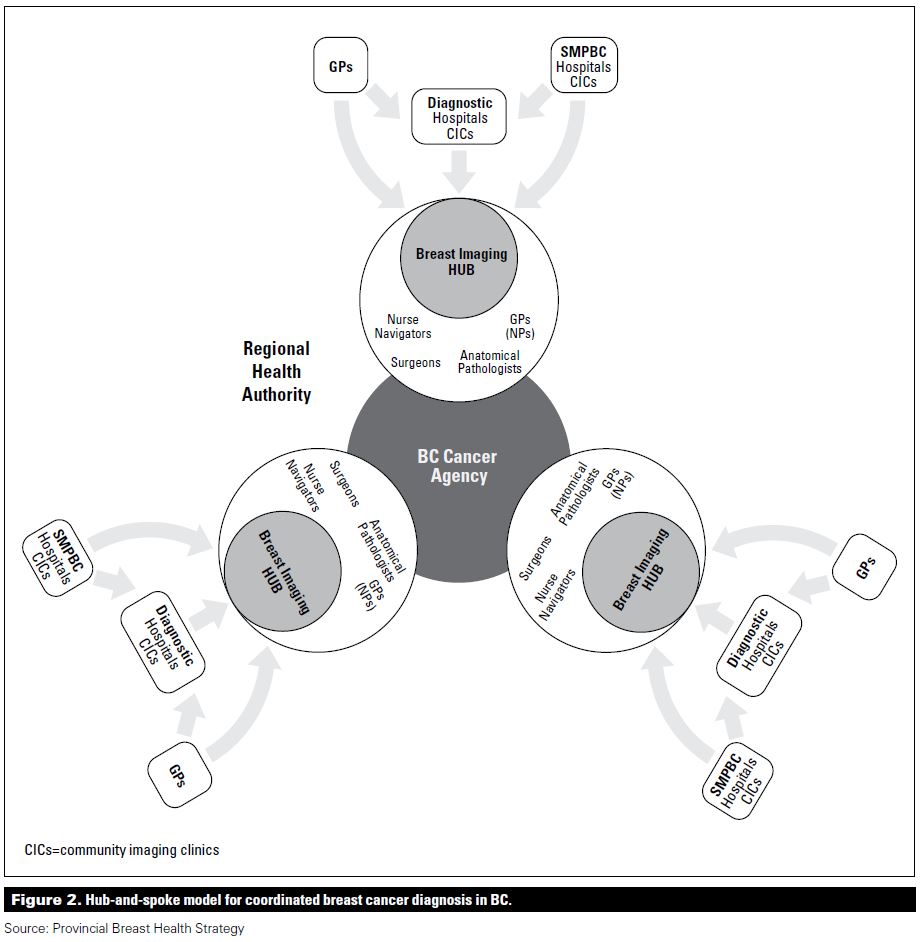
The hub-and-spoke model
The clinical pathway developed by the PBHS is based on a hub-and-spoke model, with all the necessary diagnostic services grouped or accessible so that further referrals and additional communication do not cause delays (Figure 2). This means a full-service diagnostic facility (hub) provides anatomical pathology, surgical, and oncology services to women referred directly by the SMP, family physicians, community imaging clinics, and hospitals (spokes), that may have some, but not all, of the needed services (i.e., stereotactic core biopsies, breast MRI, and MRI-guided biopsies).
It was anticipated that each HA would have three hubs. Some of these hubs would be virtual rather than physical entities, with different partners contributing services. Interconnection and communication of information were identified as vital to the model. The criteria agreed upon for each hub were as follows.
• A publicly funded medical imaging department able to provide appropriate services:
– Diagnostic mammography
– Diagnostic ultrasound
– Ultrasound-guided biopsy
– Stereotactic biopsy
– Wire localization
– Breast MRI and MRI-guided biopsy
• Accreditation for all services under the Diagnostic Accreditation Program (DAP) and the Canadian Association of Radiologists – Mammography Accreditation Program (CAR-MAP).
• A most responsible physician for all patients, facilitated by a direct link to primary care providers who accept unattached patients.
• Digital mammography equipment and related information systems (i.e., a picture archiving and communication system, a radiology information system).
• Synoptic reporting capability using Breast Imaging Reporting and Data System (BI-RADS) classification.
As well as satisfying these criteria and meeting the standard of care (image-guided core biopsy performed by radiologists using BI-RADS classification and with radiologic-pathologic correlation), each hub was expected to have the ability to:
• Audit biopsy practice.
• Coordinate multidisciplinary rounds (in person or by videoconference).
• Coordinate scheduling, referrals, patient flow, database, etc.
• Provide patients using the pathway with navigation materials and an information line for support.
• Communicate effectively with breast surgery, anatomical pathology, and BC Cancer or a hospital-based oncology program, and to do all this by direct link when not co-located with these services.
• Provide services according to available guidelines and protocols.
• Collect information required to measure performance and audit practice.[7]
Coordinated care benefits
In 2009 the Rapid Access Breast Clinic (RABC) was opened at Mount Saint Joseph Hospital using Lower Mainland innovation funding and a pay-for-performance model. Patients who presented with a breast abnormality or who had an abnormal screening mammogram at MSJ were referred to the clinic for diagnostic workup and surgery if appropriate. All investigations and appointments were coordinated by the clinic and no additional requisitions or referrals were necessary. Patients were examined by the clinic physician after diagnostic investigations and then seen to discuss correlation of the examination, imaging, and biopsy results, and for referral to the surgeon if appropriate. Clerical staff and nurse navigators helped to move patients along the clinical pathway under the supervision of clinic physicians and radiologists. In keeping with recommended guidelines, 80% of patients received a diagnosis within 21 calendar days of referral to the program.
Reductions in wait times
The effectiveness of a rapid access model of care on wait times was reviewed by comparing patients seen at the MSJ clinic with patients in the traditional system, that is, patients who had breast investigations at other centres and were then seen in an MSJ surgeon’s private office.
Patients seen at the RABC at Mount Saint Joseph waited fewer days for surgical consultation compared with patients seen at other centres (33 vs 86 days, P < .0001), and this applied to both malignant diagnoses (36 vs 59 days, P = .007) and benign diagnoses (31 vs 95 days, P < .0001).[8] Furthermore, 13% of patients in the traditional system referred to a surgeon with a benign or indeterminate diagnosis were diagnosed with breast cancer after a mean wait time of 84.2 days to see the surgeon. Of these patients, 49% presenting with benign or indeterminate diagnoses would not have been referred on to the surgeon in the RABC.
Of the patients seen at the RABC, 95% had their diagnostic studies at one centre (MSJ) and 5% had diagnostic studies at other centres. In contrast, only 61% of patients in the traditional system attended a single diagnostic centre, with 39% attending two to four diagnostic centers (P < .0001). Of the patients in the traditional system who had a diagnostic mammogram, ultrasound, and ultrasound-guided core biopsy, 31.5% attended more than one diagnostic centre.
In 2010 the Screening Mammography Program introduced fast track booking to expedite diagnostic testing following an abnormal screening mammogram. As well, many radiology facilities adopted a policy of completing diagnostic workups without requiring new requisitions for each step. Following these advances, the effectiveness of the traditional system and the coordinated care model at MSJ were assessed again in 2012 and compared. A reduction was seen in overall wait times to surgical consultation in the traditional system from 2009 (86 days) to 2012 (73 days), but the time for diagnosis for patients with cancer did not change significantly (59 vs 55 days).[9] The proportion of patients diagnosed with cancer following surgical consultation in the traditional system was reduced from 13% in 2009 to 8% in 2012. The coordinated care model at MSJ was robust over time, with a mean wait time to surgical consultation of 36 days, contrasting with 73 days in the traditional system. The time from presentation to first diagnostic imaging test, from imaging to core biopsy, and from core biopsy to surgical consultation were all reduced in the coordinated care model.
MSJ is not the only centre to have evaluated the impact of a coordinated care system. Baliski and colleagues[10] reviewed wait times to breast cancer diagnosis and surgery in 2011 in the Interior of BC. Previously, wait times in this region had exceeded targets. After the implementation of a nurse navigation program, wait times from first diagnostic imaging test to surgery were reduced from 59 to 48 days. The time from first diagnostic imaging to core biopsy and from pathological diagnosis to surgery were also reduced with coordinated care.
Cost savings
Although the Rapid Access Breast Clinic was found to reduce diagnostic wait times, there were concerns about the costs of coordinated care, so these were reviewed and compared with costs in the traditional system. Constrained by a lack of privacy agreements to allow the data sharing necessary to determine actual care costs for patients in the traditional system, an approach to modeling the costs was developed.
RABC costs were calculated by looking at clinic records for 2011 and identifying presenting complaints, the investigations conducted, and the number of visits to diagnostic imaging required to evaluate each breast problem. It was assumed that a visit to the patient’s family physician had been needed to either start the diagnostic workup or to refer the patient to the RABC.
For traditional system costs, it was assumed that each investigation and diagnostic imaging visit had required a return visit or call to the family physician to arrange the next step in the diagnostic workup or to obtain the results, as had been the case in 2009. The family physician costs were determined at the patient level using the age-appropriate MSP General Practice in-office visit fees.
Costs for RABC care were compared with the modeled costs for the traditional system, which were calculated at the patient level for the first 42 weeks of 2011 and annualized. Findings from 2009 RABC patients were also modeled and further cost savings were calculated for reduced surgical consultations for benign disease and reduced duplication of imaging costs (modeled using the cost of breast ultrasound, the least expensive investigation). The historical rate for open surgical biopsy in BC for patients presenting with a breast lump at the time of the study was 27%,[2] with a cost of $1140 compared with $582 for an ultrasound-guided core biopsy, data that were used to determine cost savings related to the improved core biopsy rate.
Costs for patient annualized physician visits were $49 554 for the RABC compared with $72 842 for the traditional system. RABC care per patient ranged from $29.79 to $44.67 compared with $29.79 to $238.32 for the traditional system. The annual cost savings in reduced surgical consults for these patients was
$55 044, and the annual cost savings in decreased duplicate breast imaging was $42 037. The annual cost savings from increasing the rate of image-guided biopsy was $153 000 in MSP costs and $176 000 in hospital costs. The total annual cost savings from the coordinated care model for patients seen at the RABC in 2011 was $448 368, which translates to a saving of $205 per patient.
Further improvements needed
In the past 5 years we have seen some clinics using the hub criteria, but the adoption of the hub-and-spoke model has been hampered by the lack of substantive permanent funding, which has resulted in the loss of services at some centres when temporary funding has dwindled or disappeared. For example, the pay-for-performance funding model that the MSJ breast clinic operated on was discontinued in 201311 and funding for nurse navigators in Kelowna was lost with budget cuts (written communication with Chris Baliski, surgical oncologist, BC Cancer Southern Interior, 4 June 2017).
Although some communication improvement has occurred between sites performing diagnostic procedures and those performing surgery, this is largely due to interest in best practice by the personnel at these sites. There has been no funding to improve data collection or communication during what has been the very slow rollout of the new Clinical and Systems Transformation (CST) information system.
While in Canada the goal has been to provide 90% of women with a definitive diagnosis based on tissue biopsy within 7 weeks,1 this has not yet been achieved in BC. The most recent figures from the Canadian Partnership Against Cancer (CPAC) for breast diagnostic wait times are from 201312 and show that 66% of BC women needing a core biopsy after an abnormal screening mammogram had the procedure within 7 weeks, while an SMP annual report including data from 201513 shows that 58% of BC women had a tissue biopsy within 7 weeks of an abnormal screening mammogram.
Over the past 5 years many Canadian provinces have implemented care pathways and navigation programs for breast diagnostics in order to meet more ambitious target wait times of 21 to 30 days from presentation to diagnosis. If there is no further improvement in BC, particularly regarding communication and navigation, our wait times for diagnostic biopsies and surgery will continue to rise well beyond what is acceptable to patients and beyond the requirements of national and international guidelines. Coordination of radiological and clinical care is needed to optimize patient experience and minimize wait times for breast cancer diagnosis.
We recommend province-wide acceptance and implementation of the PBHS so that women receive coordinated diagnostic and therapeutic care from a team of health care providers that includes medical office assistants, nurses, mammography technologists, family physicians, radiologists, surgeons, and medical and radiation oncologists
Acknowledgments
The authors would like to acknowledge the work of teams contributing to the Provincial Breast Health Strategy, particularly the Clinical Pathway Team. The authors would also like to acknowledge the contributions of Ms Lynn Pelletier, Mr Brian Schmidt, and Dr Jan Christilaw, and to thank Drs Nancy Van Laeken, Richard Lee, Sher-Ping Leung, and Carl Brown, and Ms Cheryl Bishop and Ms Shelly Fleck for assisting with data collection and analysis in the assessment of the Rapid Access Breast Clinic at Mount Saint Joseph Hospital.
Competing interests
None declared.
This article has been peer reviewed.
References
1. Provincial Breast Health Strategy. Accessed 10 July 2017. www.phsa.ca/health-professionals/data-reports/provincial-breast-health-s....
2. Screening Mammography Program. 2010 annual report. Accessed 10 July 2017. combined-files.docwww.bccancer.bc.ca/screening/Documents/SMP_Report-AnnualReport2010.pdf.
3. Five Plus. Easy steps to breast health. Accessed 10 July 2017. www.fiveplusbc.cacombined-files.doc.
4. Wilson CM. Performance indicators, 2011 to 2013. Presented at Medical Grand Rounds, Nelson, BC, 25 June 2015.
5. European Society of Breast Cancer Specialists (EUSOMA). Guidelines and publications. Accessed 10 July 2017. www.eusoma.org/Engx/Guidelines/Default.aspx?cont=default.
6. Pelletier L. Breast health strategy summary report 2012. Provincial Health Services Authority.
7. Wilson CM. Hub criteria. Presented at Medical Grand Rounds, Nelson, BC, 25 June 2015.
8. McKevitt EC, Dingee CK, Leung S, et al. Reduced time to breast cancer diagnosis with coordination of radiological and clinical care. Cureus. Published online 7 December 2017. www.cureus.com/articles/9947-reduced-time-to-breast-cancer-diagnosis-wit....
9. McKevitt E, Dingee C, Warburton R, et al. Coordination of radiologic and clinical care reduces wait times to breast cancer diagnosis. Curr Oncol 2017;24:e388-e393.
10. Baliski C, McGahan CE, Liberto CM, et al. Influence of nurse navigation on wait times for breast cancer care in a Canadian regional cancer center. Am J Surg 2014;207:686-691.
11. Chan T, Hwang H, Karimuddin A. Wait times for general surgery in BC: Moving beyond measurement. BCMJ 2015;57:341.
12. Canadian Partnership Against Cancer. Cancer system performance. Breast cancer diagnosis wait times. Accessed 15 July 2017. combined-files.docwww.systemperformance.ca/cancer-control-domain/diagnosis/breast-cancer-d....
13. Screening Mammography Program. 2016 annual report. Accessed 15 July 2017. www.bccancer.bc.ca/screening/Documents/SMP_Report-AnnualReport2016.pdf.
Dr Wilson is the director of breast imaging at BC Cancer in Vancouver and a clinical associate professor in the Department of Radiology at UBC. Drs Kuusk, Dingee, and McKevitt are surgeons at Mount Saint Joseph Hospital. In addition, Dr McKevitt is a clinical associate professor in the Department of Surgery at UBC, Dr Dingee is a clinical assistant professor, and Dr Kuusk is a clinical professor.

{kind=link}