Breast magnetic resonance imaging
Issue: BCMJ,
vol. 47 , No. 10 , December 2005 ,
Pages 543-548 Clinical Articles
Breast magnetic resonance imaging has emerged as an important new tool in the fight against breast cancer. This imaging modality is valuable when recurrence of cancer is suspected, when the extent of lobular carcinoma in situ must be determined, and when postoperative tissue reconstruction is involved. Breast magnetic resonance imaging is also a useful supplement to screening mammography when assessing high-risk women, and it is the modality of choice when determining if a silicone implant has ruptured.
The combination of anatomic and hemodynamic information provided by breast magnetic resonance imaging can be very valuable in particular clinical situations.
Breast cancer will be diagnosed in approximately 2500 women in BC this year. BC has the highest incidence of breast cancer in Canada, but it also has the best survival rate. This is due in part to improved detection of breast cancer through the Screening Mammography Program of BC, and better characterization of screen-detected abnormalities with diagnostic mammography and breast ultrasound. Screening mammography has been demonstrated to detect breast cancers before they have spread, increasing the chances that treatment will be successful. Two-thirds of screen-detected breast cancers are Stage 0 or Stage 1, with 5-year survival in excess of 95%. It is now accepted that women who have annual mammograms enjoy a survival advantage over those women who don’t. Screening mammography is the only imaging modality shown to decrease breast cancer mortality.
In spite of mammography’s proven benefits, its limitations persist. The sensitivity of mammography drops to 48% in high-density breasts.[1] Mammography is unable to completely image the lymph nodes in the axilla and to assess the blood supply to tissue. Mammography alone may not detect cancer in women who are at increased risk for the disease. In addition, this imaging technology may underestimate the true extent of the disease in a woman diagnosed with breast cancer.
Some, but not all, of these limitations may be overcome by breast ultrasound. Breast ultrasound allows radiologists to characterize abnormalities detected by mammography. For example, ultrasound can determine whether a mass seen on a mammogram is cystic and can be ignored, or is solid and may require further investigation. Ultrasound is an inexpensive and widely available technology. It is particularly useful in guiding needle biopsies. Like mammography, it also has drawbacks. While diagnostic breast ultrasound is valuable, screening breast ultrasound has never been shown to decrease breast cancer mortality (although it may prove to be useful in high-risk patients when combined with annual screening mammography). Ultrasound is operator-dependent and requires a particularly high degree of vigilance and expertise to be reliable. A properly performed survey of both breasts is time-consuming, and even in patients with biopsy-proven breast cancer, ultrasound may underestimate the size of the tumor or overlook additional foci of disease. Finally, ultrasound is of little value in the assessment of breast calcifications.
Advantages of magnetic resonance imaging
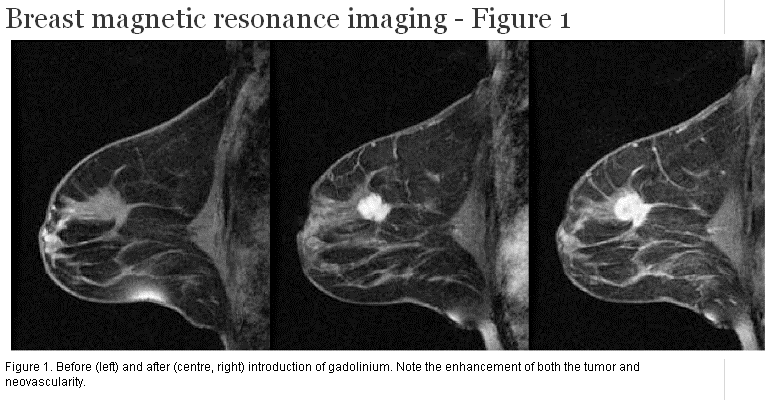
Breast magnetic resonance imaging (MRI) uses a strong magnetic field and radio frequency pulses to generate detailed three-dimensional anatomic and physiologic images of the breast and adjacent structures, which are then interpreted by radiologists. For cancer detection and preoperative assessment, it is routinely performed with gadolinium, an intravenous contrast agent. The contrast agent allows identification of neovascularity in breast tissue, an important feature that cannot be provided by current mammographic and sonographic techniques (Figure 1). In addition, rapid MR sequences can characterize the extent and kinetics of blood flow through tissue. This dynamic data may aid in the differentiation of benign and malignant lesions. This combination of anatomic and hemodynamic information is one of the strengths of breast MRI, and accounts for its greater than 98% negative predictive value. Finally, breast MR data can be reconstructed to provide the surgeon with a three-dimensional image that can serve as a road map for presurgical planning.
{kind=link}
Breast MRI can complement mammography and ultrasound. In the 12 months ending in July 2003, breast MRI was performed at approximately a dozen sites in British Columbia, including most hospitals with MR cameras. It is now widely used in the United States and Europe in the workup of mammographic and sonographic dilemmas, and may offer important additional information to the breast cancer patient and her physicians before and following treatment. The sensitivity of breast MRI for the detection of cancer is approximately 95%. It is more sensitive for invasive than in situ disease. Its specificity is reported to be as high as 73%, varying with the patient population and MR sequences employed.[2] Its positive predictive value is moderate, so a breast MR image might not obviate the need for a biopsy.[3]
One particular advantage of breast MRI is its unparalleled ability to image the chest wall. The posterior margin of a tumor deep within the breast frequently cannot be included in mammographic films, and the characteristic shadowing seen on ultrasound makes it difficult to exclude involvement of the pectoral muscles. In contrast, the field of view in a breast MR image can extend as far posteriorly as the thoracic spine, allowing the radiologist an unobstructed view of the pectoral fascia and the internal mammary lymph node chain. The large field of view also permits assessment of the supraclavicular, internal mammary, and axillary lymph nodes, as well as screening of the chest and thoracic spine for metastases (Figure 2 and Figure 3).
{kind=link}
{kind=link}
The American College of Radiology notes that there are rare situations when traditional imaging modalities are unable to guide patient management. These include situations involving inconclusive or contradictory results on mammography or ultrasound and the search for an unknown primary tumor. Breast MRI may help to solve these problems before definitive treatment. In addition to the use of breast MR images for this kind of problem-solving, the College recognizes the following as indications for breast MRI.
Appropriate breast conserving surgery hinges on accurately excluding unsuspected additional foci of disease in the breast.[4] Breast conserving surgery is most appropriate when the patient has a small, solitary index lesion. It is essential not to underestimate the extent of invasive cancer, which can happen using traditional approaches. Up to 25% of women with breast cancer will be best treated with a mastectomy because of large tumors or multifocal disease or the inability to tolerate radiation. The combination of physical examination, mammography, and breast MRI has been shown to assess the true extent of a malignancy better than other modalities, either singly or in other combinations.[5]
A significant percentage of breast cancer patients have unsuspected additional malignant disease that cannot be imaged using mammography or ultrasound. For example, unsuspected synchronous contralateral malignancies have been detected by breast MRI in 2% to 10% of patients.[6-9]
Fischer and colleagues[10] reported that in 336 patients with biopsy-proven breast cancer, MRI demonstrated unsuspected multifocal (same quadrant) foci in 8.9%, multicentric (different quadrant) foci in 7.1%, and contralateral foci in 4.5% (Figure 4). They noted that the breast MR results altered the management of 66 of these patients (19.6%), and concluded that “preoperative MR imaging of the breast is useful for staging breast carcinoma and for planning the appropriate therapy.” MRI may be particularly helpful in those patients with mammographically dense breasts, since mammography is less sensitive than MRI in these cases.[5,7,11]
{kind=link}
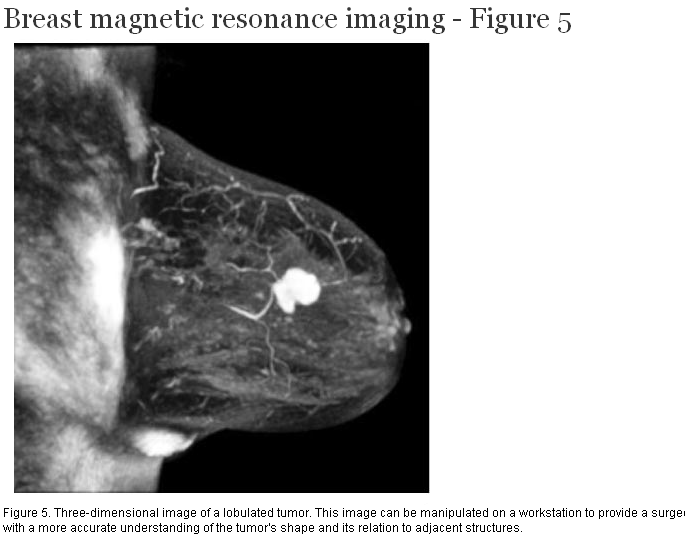
After breast conserving surgery, residual disease or close margins are sometimes found on the pathology specimen and a second operation is required. If a third operation is needed, it is usually a mastectomy. Although postoperative MRI is possible, ideally the patient must wait 6 months to permit accurate distinction between scar tissue and residual disease. This may be avoided when three-dimensional MR images of the breast tumor (or tumors) are obtained before the initial surgery[12](Figure 5).
{kind=link}
Twelve percent of patients who receive breast conserving surgery and radiation therapy develop recurrent breast cancer by 15 years.[13] Recurrences are more common in younger women, and tend to occur at the operative site.[14] Physical examination, mammography, and ultrasound may not be able to distinguish between scar tissue and a suspected recurrence, and biopsy results may be ambiguous. Breast MRI can identify recurrent disease by exploiting the fact that tumor enhances, whereas mature scar tissue does not. In this situation, it is best to perform breast MRI at least 6 months following surgery.
Neoadjuvant chemotherapy is used in a minority of breast cancer patients to decrease the size of their tumors before surgery. An important part of this strategy is to determine as soon as possible whether the chemotherapy is actually shrinking the tumor. Traditional approaches such as palpation, mammography, and ultrasound are insensitive, and are often unable to distinguish between a shrinking tumor and the adjacent inflammation and scarring. Breast MRI is a very sensitive modality for determining whether a particular neoadjuvant regimen is having the desired effect.[15]
Mammography is less sensitive for invasive lobular carcinoma than for invasive ductal carcinoma, regardless of the breast density.[4] Invasive lobular carcinoma is also difficult to detect by physical exam and ultrasound. It is bilateral in 10% of cases, and is multifocal and multicentric in up to 40% of patients. It is a common cause of positive margins on resection specimens. MRI is better able to determine the extent of invasive lobular carcinoma than mammography, and in one study altered the management of 50% of 32 women with invasive lobular carcinoma.[16]
Postoperative tissue reconstruction
Imaging of transverse rectus abdominis myocutaneous (TRAM) flap reconstruction following mastectomy poses a particular challenge to the mammographer and sonographer because of postoperative distortion and the fact that recurrences tend to involve the chest wall. Breast MRI’s superior assessment of the chest wall overcomes these limitations.
Annual mammography remains the gold standard for breast cancer screening, and the BC Cancer Agency recommends that women aged 40 to 79 have a screening mammogram at least every 2 years. Breast MRI is not a suitable screening tool for the general population because of time constraints, expense, and high rate of false-positives, but it shows promise as a supplemental screening tool for patients who are at increased risk for breast cancer, particularly those with dense breasts on mammography. These include BRCA1 and BRCA2 mutation carriers, patients with a strong family history of breast cancer, breast cancer patients, and patients who received radiation therapy for Hodgkin disease as adolescents.
BRCA1 and BRCA2 carriers have cumulative lifetime risk of breast cancer of 85%.[17] Tumors in women with BRCA1 tend to be invasive, yet appear more benign on mammography than typical cancers, hindering their detection and assessment by mammography and ultrasound. These women often develop cancer at a much younger age than the general population when their breast tissue is still quite dense. Screening breast MRI is more sensitive (77%) than mammography (36%), ultrasound (33%), or physical examination alone (9%) in these patients.[18]
There is no consensus on the best screening protocol for high-risk women. One suggestion is to alternate screening mammography with screening breast MRI at 6-month intervals.
Although no registry is kept, it is thought that more than 20 000 women in British Columbia have had a breast augmentation procedure. Prostheses consist of an outer silicone shell containing saline, gel-like silicone, or both. When saline-containing implants rupture they usually deflate completely because of the rapid absorption of saline by the bloodstream. Ruptured silicone-containing implants do not deflate in this way and are thus more difficult to assess on physical examination. Breast MRI is the imaging modality of choice when trying to determine whether a silicone-containing implant has ruptured.
Breast MRI is an important new adjunct to physical examination, mammography, and ultrasound in the evaluation of breast cancer. It is helpful in the workup of patients with a suspected recurrence, invasive lobular carcinoma, or TRAM flap reconstruction. It will not replace mammography as a screening modality for the general population, but should be considered as a supplement to screening mammography in high-risk women. It is the gold standard for assessment of suspected silicone implant ruptures.
Should all newly diagnosed breast cancer patients have routine MRI before treatment? Recurrence rates are significantly lower in women who have had preoperative breast MRI.[19] Breast MR images can detect unsuspected additional tumors in these patients, can prevent understaging the disease, and can improve surgical planning. It is not yet known whether detecting these additional tumors will result in improved survival. Some have argued that the additional tumors found by MRI are nonlethal or will be killed by the radiation therapy or chemotherapy the patient may receive later.[20] Furthermore, most sites in British Columbia lack the ability to perform breast biopsies under MRI guidance. This is a potential drawback when a lesion is seen only by MRI (although a “second look” ultrasound might be able to locate the lesion for an ultrasound-guided biopsy). Nevertheless, more accurate staging cannot help but lead to better outcomes.[21] Based on the available data and the indications adopted by the American College of Radiology, it is reasonable to consider preoperative MRI for all newly diagnosed breast cancer patients, and particularly those who have dense, nonfatty breasts on mammography, invasive lobular carcinoma, or an extensive intraductal component on the initial biopsy.
Competing interests
None declared.
References
1. Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: An analysis of 27,825 patient evaluations. Radiology 2002;225:165-175. PubMed Abstract
2. Hlawatsch A, Teifke A, Schmidt M, et al. Preoperative assessment of breast cancer: Sonography versus MR imaging. AJR 2002;179:1493-1501. PubMed Abstract Full Text
3. Bluemke DA, Gatsonis CA, Chen MH, et al. Magnetic resonance imaging of the breast prior to biopsy. JAMA 2004;292:2735-2742. PubMed Abstract Full Text
4. Osteen RT. Selection of patients for breast-conserving surgery. Cancer 1994;74:366-371. PubMed Abstract
5. Berg WA, Gutierrez L, NessAiver MS, et al. Diagnostic accuracy of mammography, clinical examination, US, and MR imaging in preoperative assessment of breast cancer. Radiology 2004;233:830-849. PubMed Abstract
6. Hungness ES, Safa M, Shaughnessy EA, et al. Bilateral synchronous breast cancer: Mode of detection and comparison of histologic features between the two breasts. Surgery 2000;128:702-707. PubMed Abstract Full Text
7. Sardanelli F, Giuseppetti GM, Panizza P, et al. Sensitivity of MRI versus mammography for detecting foci of multifocal, multicentric breast cancer in fatty and dense breasts using the whole-breast pathologic examination as a gold standard. AJR 2004;183:1149-1157. PubMed Abstract Full Text
8. Liberman LL, Morris EA, Kim CM, et al. MR imaging findings in the contralateral breast of women with recently diagnosed breast cancer. AJR 2003;180:333-341. PubMed Abstract Full Text
9. Lee SG, Orel SG, Woo IJ, et al. MR imaging screening of the contralateral breast in patients with newly diagnosed breast cancer: Preliminary results. Radiology 2003;226:773-778. PubMed Abstract Full Text
10. Fischer U, Kopka L, Grabbe E. Breast carcinoma: Effect of preoperative contrast-enhanced MR imaging on the therapeutic approach. Radiology 1999;213:881-888. PubMed Abstract Full Text
11. Esserman L, Hylton N, Yassa L, et al. Utility of magnetic resonance imaging in the management of breast cancer: Evidence for improved preoperative staging. J Clin Oncol 1999;17:110-119. PubMed Abstract Full Text
12. Lee JM, Orel SG, Czerniecki BJ, et al. MRI before reexcision surgery in patients with breast cancer. AJR 2004;182:473-480. PubMed Abstract Full Text
13. Fisher ER, Anderson S, Tan-Chiu E, et al. Fifteen-year prognostic discriminants for invasive breast carcinoma. Cancer 2001;91:1679-1687. PubMed Abstract Full Text
14. Bartelink H, Horiot JC, Poortmans P, et al. Recurrence rates after treatment of breast cancer with standard radiotherapy with or without additional radiation. N Engl J Med 2001;345:1378-1387. PubMed Abstract Full Text
15. Erlemann R. Dynamic, gadolinium-enhanced MR imaging to monitor tumor response to chemotherapy. Radiology 1993;186:904-905. PubMed Citation
16. Weinstein SP, Orel SG, Heller R, et al. MR imaging of the breast in patients with invasive lobular carcinoma. AJR 2001;176:399-406. PubMed Abstract Full Text
17. Ford D, Easton DF, Stratton M, et al. Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer families. Am J Hum Genet 1998;62:676-689. PubMed Abstract Full Text
18. Warner E, Plewes DB, Hill KA, et al. Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004;292:1317-1325. PubMed Abstract Full Text
19. Fischer U, Zachariae O, Baum F, et al. The influence of preoperative MRI of the breasts on recurrence rate in patients with breast cancer. Eur Radiol 2004;14:1725-1731. PubMed Abstract Full Text
20. Kneeshaw PJ, Turnbull LW, Drew PJ. Current applications and future direction of MR mammography. Br J Cancer 2003;88:4-10. PubMed Abstract Full Text
21. Liberman L, Morris EA, Dershaw DD, et al. MR imaging of the ipsilateral breast in women with percutaneously proven beast cancer. AJR 2003;180:901-910. PubMed Abstract Full Text
Ian Gardiner, MD, FRCPC, Urve Kuusk, MD, FRCPC, Bruce Forster, MD, FRCPC, Audrey Spielmann, MD, FRCPC
Dr Gardiner is a clinical assistant professor in the Department of Radiology at the University of British Columbia and a director of the Advanced Breast Imaging Program at the Canada Diagnostic Centre. Dr Kuusk is a clinical associate professor in the Department of Surgery at UBC. Dr Forster is an associate professor in the Department of Radiology, Faculty of Medicine, at UBC. He is also a staff radiologist at UBC Hospital and medical director of Canada Diagnostic Centres (BC). Dr Spielmann is an assistant professor in the Department of Diagnostic Radiology at UBC, a staff radiologist at Vancouver Coastal Health, Vancouver Acute, and University Hospital sites, and a consultant for Canada Diagnostic Centre with a special interest in breast and abdominal MRI.