Aspirated foreign bodies in children: BC Children’s Hospital emergency room protocol
Issue: BCMJ,
vol. 50 , No. 5 , June 2008 ,
Pages 252-256 Clinical Articles
Foreign bodies lodged in either the larynx or bronchi lead to significant morbidity and mortality in children. Diagnosis may be delayed for several reasons. Often parents or caregivers do not recognize that a choking event has occurred. Symptoms often mimic asthma or croup. Standard radiographic examinations may not reveal the foreign body. As well, medical schools and residency programs do not consistently provide formal education on the diagnosis of foreign body aspiration. Clinicians should be aware that diagnosis of foreign body aspiration requires a history, a physical examination, and, in the case of non-metallic bronchial foreign bodies, special imaging (prior to the onset of atelectasis and pneumonia, inspiratory and expiratory chest radiographs may reveal obstructive emphysema). If a bronchial foreign body is suspected, rigid laryngobronchoscopy should be performed by a team of medical professionals with proper experience and equipment. If a laryngeal foreign body is suspected, flexible laryngoscopy may be diagnostic; definitive treatment requires rigid laryngoscopy under general anaesthesia.
Delays in diagnosing upper aerodigestive objects in children may be avoided by obtaining a history, performing a physical examination, and reviewing inspiratory and expiratory chest radiographs.
Aspiration of foreign bodies results in significant morbidity and mortality in children. The majority of foreign body aspirations occur in children younger than 4 years of age.
Immature dentition, poor food control, physical activity during feeding, and propensity to explore the environment orally all make children susceptible to foreign body aspiration.[1]
In the first 9 months of 2007, the divisions of emergency medicine and otolaryngology at BC Children’s Hospital (BCCH) treated nine children with a bronchial or esophageal foreign body after diagnosis had been significantly delayed. In five patients, a bronchial foreign body eluded diagnosis for at least 3 weeks.
Nut fragments were eventually found in four toddlers and a thumbtack was found in one teenager. Four of these patients presented to BCCH in September 2007. The parents of all five patients had already reported to one or more physicians outside BCCH that their child had experienced a coughing fit after oral exposure to a nut or a thumbtack.
Prior to referral to BCCH, the patients had received various medications and some had multiple hospital admissions. Radiology confirmed our clinical suspicions. In the OR, all five patients were found to have severe purulent bronchitis and bronchial granulation tissue formation, which made removal of the foreign bodies by rigid bronchscopy more difficult than usual.
All patients needed postoperative antibiotics and one toddler needed postoperative overnight ICU care. Fortunately, no patient needed a thoracotomy and all recovered fully.
We believe that education regarding the diagnosis and treatment of upper aerodigestive foreign bodies is a responsibility that should be shared between medical schools and university departments of otolaryngology, emergency medicine, pediatrics, and family medicine. We recognize that there are numerous factors that might cause delays in diagnosis.
These include the following:
• Lack of parent or caregiver recognition of the choking event.
• Parental denial.
• Unwarranted reassurance provided by medicines that cause temporary improvement of signs and symptoms.
• Difficulty performing radiographic examinations for radiolucent foreign bodies.
• Difficulty distinguishing coins from disc batteries radiographically.
• Lack of consistent formal education regarding injuries caused by aspirated foreign bodies in many medical schools and residency programs.
In order to reduce the morbidity associated with delayed diagnosis and to establish consistency in evaluation of children with aspirated foreign bodies, we have developed the following guidelines for BC physicians. We are also working to complete two interactive computerized learning modules: one on bronchial foreign bodies and another on esophageal foreign bodies.
In addition we plan to develop a learning module on obstructive and nonobstructive laryngeal foreign bodies. We plan to make these modules available free of charge to medical schools and residency programs and will try to promote their worldwide implementation.
While treatment is our focus here, prevention is key. Parents should be warned of the risk of death to young children from uncut hot dogs, uncut grapes, gel candies (“fruit poppers”), popped balloons, and disc batteries. Hot dogs and grapes should be cut into small pieces until a child is at least 5 years old and has no developmental delay in terms of swallowing.
Children should be taught to sit quietly while chewing and swallowing. A child’s diet should be advanced slowly in terms of food textures.[2] We look forward to continuing to educate the public about choking hazards and prevention through Safe Start, BCCH’s injury prevention program.
Because it is difficult to convince most adults of the realities of choking hazards, we plan to develop a web-based educational video and an interactive web site on choking risks, prevention, and treatment that is geared toward preteens, teenagers, parents and teachers, day-care staff, and babysitting course instructors. We hope these materials will change society’s perception of choking and thus reduce choking morbidity and mortality.
Laryngeal foreign bodies
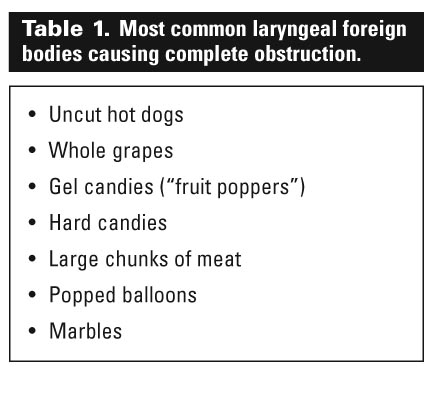
Completely obstructive laryngeal foreign bodies cause acute respiratory distress and aphonia. Uncut hot dogs, uncut grapes, and gel candies are the foods most commonly responsible for lethal choking (Table 1). Retrieval of these objects requires prompt basic life support measures, such as the Heimlich maneuver or rigid laryngoscopy and retrieval with McGill forceps.
In older children, heroic maneuvers, such as cricothyroidotomy or rapid tracheotomy (or both) can be technically possible and may allow bypass of the obstructed larynx.[3]
Partially obstructive laryngeal foreign bodies include thin, sharp objects, such as metallic stickers (Table 2). On rare occasions, these objects can become lodged between the vocal cords in the sagittal plane and cause dysphonia, a croupy cough, and progressive biphasic stridor despite medications for presumed croup.
Flexible laryngoscopy is often needed to identify radiolucent objects. Occasionally a large metal object, such as a fishhook, may become a partially obstructive supraglottic foreign body. This is usually readily diagnosed by history and radiology.[4]
Bronchial foreign bodies
Aspirated foreign bodies most commonly lodge in the bronchi. Organic objects, especially nut fragments, account for the majority of aspirated objects (Table 3). Inorganic objects, such as plastic toy parts and metal pins and thumbtacks, account for the rest.[5]
Diagnosis of bronchial foreign body aspiration is challenging in children[6] and delayed diagnoses occur for several reasons. The aspiration event is often unwitnessed or denied by parents. Most aspirated objects are radiolucent. After the initial coughing paroxysm, there is usually a quiescent (relatively asymptomatic) phase for about a week before pneumonia or other complications occur.
The wheezing that is present during the quiescent phase is often attributed to viral infections or asthma and may initially respond to bronchodilators, steroids, or antibiotics. Every year at BCCH we encounter several cases in which the diagnosis of a bronchial foreign body has been delayed, sometimes for several weeks or longer.
Potential complications of untreated bronchial foreign bodies include atelectasis, pneumonitis, bronchial granulomas, recurrent pneumonias, pneumomediastinum, bronchiectasis, plastic bronchitis, and bronchocutaneous or bronchovascular fistulization.
A high index of suspicion is required for prompt diagnosis.[7] Any patient who has a severe coughing fit after oral exposure to a high-risk object should be considered to have a bronchial foreign body until proven otherwise.[8]
Pathophysiology
Pathophysiological considerations for aspirated foreign bodies include the anatomy of the lodgment site, the physical properties of the foreign body (size, shape, and composition), and the local tissue reaction to the foreign body. For example, eggshells have a propensity to obstruct the larynx because their sharp, thin, and firm nature allows them to lodge between the vocal cords in the sagittal plane.
The specific physical property of the object and the local reaction determine the risk category of the aspirated foreign body. High-risk objects create more morbidity than the low-risk objects.[9]
High-risk objects include any small hard pieces of food, especially nuts or nut fragments, seeds, raw carrots, raw apples, raw pears, unpopped popcorn kernels, dried peas or beans (which expand rapidly as they absorb moisture and therefore require urgent bronchoscopic removal), or any small pieces of toys, plastic, metal, pebbles, stones, or beads. Low-risk objects include processed dried cereal, wet noodles, chips, pretzels without nuts, soft or pureed foods, and cheese.
Evaluation
Three important diagnostic procedures help determine the need for bronchoscopy: history, physical examination, and imaging. A history of choking is present in 75% to 90% of cases. Obtaining a history of choking is therefore essential to the diagnosis of aspirated foreign bodies.
An airway foreign body should be suspected if a child puts an object into his or her mouth and then experiences paroxysmal coughing for at least 1 minute. While a severe coughing fit suggests an airway foreign body, gagging and retching without coughing suggest a pharyngeal or esophageal foreign body.
Physical examination is nonspecific and often the findings are similar to those for a child with reactive airway disease. The classic triad of wheeze, cough, and decreased breath sounds occurs in only one-third of all cases. This triad is more common when diagnosis is delayed. About 20% of patients with bronchial foreign bodies are totally asymptomatic.
Inspiratory and expiratory chest radiographs are difficult to obtain in an uncooperative child. Despite this, in some series, up to 80% of retrieved bronchial foreign bodies demonstrated abnormal inspiratory and expiratory chest radiographs (Figure 1). Lateral decubitus chest radiographs and fluoroscopy are rarely used at BCCH, but may be helpful for diagnosis in less cooperative children.[10]
Treatment
Once a bronchial foreign body is identified, rigid bronchoscopy is almost always successful in retrieving the aspirated object (see Figure 2). For affected children, care at a tertiary centre with a full array of pediatric bronchoscopic and anesthetic equipment and expertise is highly recommended.[11]
Stable children suspected of unilateral foreign body aspiration are all candidates for bronchoscopy. However, the BC Children's Hospital Aspirated Foreign Body Protocol should not be used in the following circumstances:*
• Upper airway aspirations, including laryngeal or pharyngeal aspirations presenting with upper airway obstruction signs and symptoms, including stridor, croupy cough, hoarseness, and aphonia.
• Bilateral bronchial foreign body aspiration.
• Clinically unstable children with decreased level of consciousness, airway compromise, respiratory failure (abnormalities of oxygenation and ventilation), or shock.
Conditions that preclude rigid laryngoscopy (such as cervical spine instability, mandibular hypoplasia and macroglossia or glossoptosis) also preclude the use of this protocol; in such cases, flexible endoscopy and intubation and/or temporary tracheotomy or bronchotomy might be needed to facilitate diagnosis, patient ventilation, and airway foreign body removal.†
Summary
Evaluations of foreign body aspiration requires a history, a physical examination, and imaging. A history suggestive of foreign body aspiration includes a witnessed episode of choking or acute respiratory distress. The physical examination should focus on identifying the presence of a focal wheeze or poor aeration, and inspiratory and expiratory chest radiographs should be used to look for air trapping on expiration or unilateral atelectasis.
Suggestive findings in two of the three evaluation categories (history, physical examination, and imaging) require involvement of a pediatric otolaryngologist for rigid bronchoscopy. (If a pediatric otolaryngologist is not available, the surgeon with the most experience with rigid pediatric bronchoscopy and foreign body removal should be consulted.)
Suggestive findings in one of the three evaluation categories require consultation with a pediatric otolaryngologist and close follow-up. Equivocal findings of any kind require close follow-up.
Dedication
Dr Ludemann dedicates this work to the memory of Dr Michael F. Smith, esteemed anesthesia colleague and friend.
Competing interests
None declared.
*Corrected 3 July 2008
† Added 3 July 2008
References
1. Ayed A, Jafar AM, Owayed A. Foreign body aspiration in children: Diagnosis and treatment. Pediatr Surg Int 2003;19:485-488.
2. Rovin J, Rodgers B. Pediatric foreign body aspiration. Pediatr Rev 2000;21:86-90.
3. Morley RE, Ludemann JP, Moxham JP, et al. Foreign body aspiration in infants and toddlers: Recent trends in British Columbia. J Otolaryngol 2004;33:37-41.
4. Oguz F, Citak A, Unuvar E, et al. Airway foreign bodies in childhood. Int J Pediatr Otorhinolaryngol 2000;52:11-16.
5. Midulla F, Guidi R, Barbato A, et al. Foreign body aspiration in children. Pediatr Int 2005;47:663-668.
6. Chiu CY, Wong KS, Lai SH, et al. Factors predicting early diagnosis of foreign body aspiration in children. Pediatr Emerg Care 2005;21:161-164.
7. Metrangelo S, Monetti C, Meneghini L, et al. Eight years’ experience with foreign-body aspiration in children: What is really important for a timely diagnosis? J Pediatr Surg 1999;34:1229-1231.
8. Even L, Heno N, Talmon Y, et al. Diagnostic evaluation of foreign body aspiration in children: A prospective study. J Pediatr Surg 2005;40:1122-1127.
9. Schmidt H, Manegold BC. Foreign body aspiration in children. Surg Endosc 2000;14:644-648.
10. Schunk JE. Foreign body—ingestion/aspiration. In: Fleisher GR, Ludwig S, Henretig FM, (eds). Textbook of Pediatric Emergency Medicine. 5th ed. Philadelphia: Lippincott Williams and Wilkins; 2006:307-314.
11. Ludemann JP, Hughes CA, Holinger LD. Management of foreign bodies of the airway. In: Shields TW, LoCicero J, Ponn RB (eds). General Thoracic Surgery. Vol. 1. 5th ed. Philadelphia: Lippincott Williams and Wilkins; 2000:853-862.
Dr Dehghani is a physician in the Division of Pediatric Emergency Medicine at BC Children’s Hospital and a clinical associate professor in the Department of Pediatrics at the University of British Columbia. Dr Ludemann is an otolaryngologist in the Division of Pediatric Otolaryngology at BC Children’s Hospital and a clinical assistant professor in the Department of Surgery at UBC.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}