By: Ian Courtice, MD, Ken Hughes, MD,
BC specialists travel to Cleveland Clinic, one of the world’s foremost medical centres
Issue: BCMJ,
vol. 55, No. 1, January February 2013,
Pages 44,49 Specialist Services Committee
What does the Cleveland Clinic have to do with health care in BC?
Well, the two of us traveled to Ohio with a group of BC specialists and health care executives in November to find out.
The not-for-profit Cleveland Clinic is one of the top three medical centres in the US, receiving accolades around the world for its patient-first approach to medicine.
While the clinic is known for many medical landmarks including the first coronary bypass surgery, the first larynx transplant, and the discovery of the coronary angiography, it is the culture of the clinic that makes the biggest impact on physician and staff work life and patient health care.
It’s a true service-oriented culture with everything organized to be fully accommodating to the patient or visitor. Upon walking through the front door someone is there to greet you, ensuring no one is wandering around lost or confused. The staff wear color-coded jackets so patients know who’s who—greeters wear red jackets, and doctors wear the traditional white lab coat.
The goal of the excursion was to study a quality-driven organization that delivers world-class, patient-first health care. The tour was organized by the Practice Support Program in collaboration with the Specialist Services Committee.
The BC team got extraordinary access with briefings from a full roster of Cleveland Clinic executives and managers including President and CEO Dr Delos M. Cosgrove.
We discovered that many of the best practices happening at the Cleveland Clinic are completely transferable to BC. They look after the same types of patients and have similar process issues. If funding could truly follow the patient in the BC system then the cultural innovations of the Cleveland Clinic could also be used here.
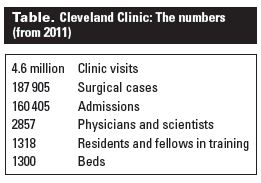
In Canadian terms the Cleveland Clinic is not a clinic at all. It’s a first-class hospital, research facility, and medical school all rolled into one. It employs 36000 people including 2857 physicians and scientists. In practical terms it has much in common, albeit on a smaller scale, with BC’s health system.
In its 91-year history the Cleveland Clinic has shown a clear pattern of breaking from traditional thinking, including adopting a strong emphasis on specialized medicine long before it was vogue.
Other innovations include:
• A vision to “re-humanize” the hospital experience.
• The creation of institutes to deliver care in a way easily understood by patients (e.g., Heart & Vascular Institute, Digestive Disease Institute).
• A system of all physicians being salaried and on 1-year contracts. Contracts are renewed based on performance.
• A physician-led board of governors. Physicians also lead the executive team and steer the direction of the center.
• A significant focus on metrics. As stated by Chief Medical Operations Officer Dr Robert Wyllie, “If you can’t measure it, you can’t manage it.”
Another element that stood out to us while touring the clinic was the extremely focused leadership of the Cleveland Clinic executives. A few years ago the physician-led executive team realized that although their patient outcomes were exceptional, they were failing to measure up in patient satisfaction surveys.
They set a plan in motion to improve their scores based on several simple initiatives, including a new, simple policy that introduced quiet hours in the evenings. Within 3 years, patient satisfaction scores rose from 46% to 92%.
The key revelation uncovered by this simple change was that as patient satisfaction improved, so did provider satisfaction. Strong leadership and measurable initiatives make all the difference.
As well as the high level of provider satisfaction, the attitude of the staff was notable. They clearly love going into work every day. They’re not there because of the money; they’re there because of the culture.
A second visit to the clinic with a different group of specialist physicians is planned for early this year. The focus of this trip will be to look at practical applications and the degree to which elements of the clinic’s programs could work for BC’s specialist physicians. A review will be published in this column.
For more information, visit the Cleveland Clinic website at www.clevelandclinic.org.
—Ian Courtice, MD
—Ken Hughes, MD
This article is the opinion of the SSC and has not been peer reviewed by the BCMJ Editorial Board.