Removal of ear canal foreign bodies in children: What can go wrong and when to refer
Issue: BCMJ,
vol. 51 , No. 1 , January February 2009 ,
Pages 20-24 Clinical Articles
Two cases illustrate the difficulty of removing ear canal foreign bodies that are large, ungraspable, or both. Early referral should be considered in such cases, since multiple attempts at foreign body removal are associated with increased risk of pain, bleeding, patient anxiety, loss of cooperation, and serious otologic complications. Successful ear canal foreign body removal requires optimal visualization, proper instruments, and appropriate techniques. Depending on the object, its location within the ear canal, and the level of patient cooperation, it might be appropriate to use a right-angled hook, otologic forceps, suction, mineral oil, water irrigation, or a drop of cyanoacrylate (superglue) on the wooden end of a cotton-tipped applicator. An individualized approach should be adopted to determine which cases can likely be managed in the emergency room and which cases warrant early referral to an otolaryngologist.
While the majority of objects lodged in the ear canal can be removed without referral to an otolaryngologist, complex cases can result in significant morbidity and should be referred.
The management of ear canal foreign bodies (ECFB) in children can be challenging. Many ECFB, including pebbles, beads, and other small objects, are readily removed by general practitioners and emergency physicians. Occasionally an ECFB is difficult to remove and requires the use of specialized approaches and techniques or referral to an otolaryngology service, as the following two cases illustrate.
Case data
In case 1, an 8-year-old female was brought to the emergency room after placing a smooth plastic bead in her left ear canal. The hollow bead was shaped like a lifesaver and had become wedged against the ear canal skin circumferentially. An unsuccessful attempt was made to remove the bead with the patient under general anesthesia (GA). When the patient awoke from the GA with vertigo and left hearing loss, she was referred to Pediatric Otolaryngology at BC Children’s Hospital.
Upon arrival at BCCH the following day, the patient had no nystagmus or facial weakness. After a blood clot was aspirated during examination of the ear with the patient under GA, the bead was found lodged tightly and completely within the middle ear, medial to the handle of the malleus, which had been fractured medially. With much difficulty the bead was tilted away from the stapes in an anteriorinferior direction and removed using a right-angle hook [Figure 1]. This procedure took about 20 minutes. Reinspection showed that 80% of the tympanic membrane was missing. The incus and stapes were obscured by the tympanic remnant, mucosal edema, and blood. The patient was treated with ciprofloxacin and dexamethasone otic (Ciprodex drops).
The next day a pure tone audiology assessment revealed a mild to moderate left conductive hearing loss with mild left sensorineural hearing loss. Hearing in her right ear was normal.
The patient was examined again under GA 2 weeks later. Microotoscopy revealed a 70% tympanic perforation and a small posteroinferior medial ear canal web, which was then divided. There was no growth of squamous epithelium in the middle ear. The patient experienced intermittent vertigo for 2 months and headaches for 3 months post-op. At that time the patient still had mild to moderate conductive hearing loss in the left ear. A large perforation of the left tympanic membrane was observed, and ossicular chain disruption was suspected. The patient was given a hearing aid and preferential seating in her classroom. Despite water precautions the patient had several episodes of purulent left otorrhea, which were treated effectively with Ciprodex drops. Tympanoplasty was performed 9 months after the initial injury; the middle ear was found to be dry, but there was granulomatous tissue within the posterosuperior ear canal and covering the incus long process, stapes, and oval window. There was also blunting of the posterior annular angle and there were posteroinferior middle ear scar adhesions. Four months after tympanoplasty, the patient was found to have a much smaller tympanic perforation and a slight to mild conductive hearing loss. Her hearing aid has been adjusted and further surgery will be considered if the perforation does not heal completely.
In case 2, a 6-year-old female presented to the ER with a popcorn kernel in her ear. Initial attempts to remove the kernel with a curette were unsuccessful. An attempt was then made to remove the kernel by applying cyanoacrylate (superglue) to the wooden end of a cotton-tipped swab and inserting this into the ear canal. Unfortunately, the glue made the kernel adhere to the ear canal skin. Subsequent microotoscopy in the pediatric otolaryngology clinic revealed that the dried glue and popcorn kernel formed a 95% middle ear canal obstruction. There was no space to insert a right-angle hook to extract the foreign body complex. Since the patient already had a surgery date for another elective procedure 9 days later and had no pain or inflammation from the foreign body, ECFB removal was planned for the upcoming GA. The night before the surgery the patient’s father saw a portion of the glue at her auricular meatus, grasped this with his fingers, and removed the glue and popcorn kernel together in one piece [Figure 2].
{kind=link}
The next day the residual ear wax was removed under GA and there was no evidence of any foreign body remnants or trauma to her ear canal or tympanic membrane.
Discussion
“Adequate visualization, appropriate equipment, a cooperative patient, and a skilled physician are the keys to successful foreign body removal.”[1] Along with these requirements, the literature identifies numerous specific risk factors for complications of ear canal foreign body removal.
The old adage “If at first you don’t succeed, try, try again” certainly does not apply to removing objects from children’s ears. Multiple attempts at ECFB removal are associated with increased risk of pain, bleeding, patient anxiety, loss of cooperation, and serious otologic complications. Uncommon but potential otologic complications of ECFB removal include ossicular chain damage, sensorineural hearing loss, vertigo, facial nerve paralysis, and meningitis.
Marin and Trainor found that in 244 ER patients with ECFB, 80% had the foreign body removed successfully by emergency physicians and 12% experienced complications. Failure to remove the ECFB and complications secondary to ECFB removal were both associated with multiple attempts at removal and the use of multiple instruments. Of those patients subsequently referred to an otolaryngology service for removal, 26 foreign bodies were removed in the otolaryngology clinic while 14 were removed in the OR. This study concluded that referral to otolaryngology should be considered when more than one attempt or more than one instrument is needed to remove an ECFB.[2] After examining 738 ECFB cases, Singh and colleagues drew the somewhat radical conclusion that an otolaryngology service should be involved in the management of all ECFB cases.[3] Clearly this conclusion is not compatible with the current standard of practice in BC, where many ER physicians have become skilled at removing foreign bodies in uncomplicated cases.
Challenges
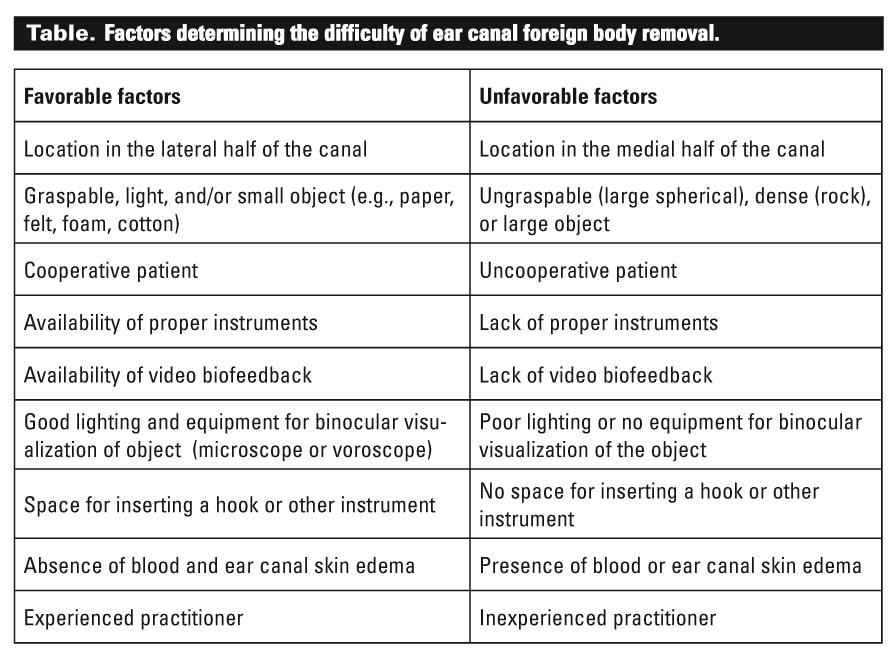
The difficulty of ear canal foreign body removal depends on several factors [Table], including whether the object is in the lateral or medial half of the ear canal, and whether the object is difficult or easy to grasp. Both the failure to remove an ECFB and increased complication rates have been associated with objects that are difficult to grasp. One study found that easy-to-grasp objects had a successful removal rate of 64% and a complication rate of 14%, while difficult- to-grasp objects had a successful removal rate of 45% and a complication rate of 70%.[4] Difficult ECFB removals have also been associated with objects that are spherical, that touch the tympanic membrane, and that have been in the canal for more than 24 hours.5 ECFB removal can be challenging when the object completely obstructs the ear canal or is caustic or pro-inflammatory (sharp or causing an allergic reaction), or when previous attempts at removal have resulted in ear canal laceration, otitis externa, or both. We have found that most small, inert foreign bodies can be observed for 1 to 2 weeks without increased complications. Button-type disc batteries, however, require urgent removal, and patients with these caustic foreign bodies may present with swelling, ulceration, and dark otorrhea.[2,6,7] Live insects can often be removed by turning off room lights, then luring the insect out using a flashlight, or alternatively, by drowning the insect in saline or oil, then applying suction.
{kind=link}
High-risk ECFB situations appropriate for referral to an otolaryngology service can be identified based on the characteristics of the foreign body, its relative size and location within the ear canal, the presence of trauma to the canal, and the number of attempts already made.[1] While the majority of foreign bodies are removed without serious consequences, complex cases require cautious management given the potential morbidity associated with failed attempts at ECFB removal.
Approaches and techniques
A variety of approaches exist for removing the diverse array of foreign bodies that find their way into children’s ear canals. All of these require optimal visualization of the foreign body, which is best achieved using the excellent light and magnification afforded by a binocular microscope. One of the authors (JPL) routinely uses binocular microscopic visualization with video feedback via a TV monitor to decrease the patient’s fear of the unknown, to alleviate anxiety, and to improve cooperation.[8]
A voroscope (e.g., LumiView) is a moderate-cost alternative that permits “tunneled” binocular vision with less magnification but with more maneuverability. This is useful for less cooperative patients and for settings outside the otolaryngology clinic. Given the expense and limited availability of magnification and lighting equipment, a relatively low-cost alternative is a standard headlamp from an outdoor equipment store.
Techniques for ECFB removal rely on various instruments and aids, including the right-angle hook, otologic forceps, and cynanoacrylate (superglue) on the wooden end of a cotton-tipped applicator.
• Right-angle hook. This instrument is particularly helpful for spherical objects, which cannot usually be captured with a wire loop or ear curette. The tip of the hook should be advanced beyond the equator of the object in the anteriorsuperior region of the canal, then carefully withdrawn in a posteroinferior direction to avoid ossicular trauma. Note that this technique often causes a minor skin laceration, which can be treated effectively using a single instillation of antibiotic eardrops with or without xylometazoline (Otrivin), which is safe otologically and hemodynamically, based on extensive experience during bilateral myringotomy and tympanostomy tube insertion. The authors have never seen tympanic membrane trauma from the technique, but this is a potential risk, especially without GA. If the foreign body is a bead with a hole in it, the tip of a short right-angle hook can usually be inserted into the hole and the bead can be easily removed. Some physicians have used a bent paperclip in place of a right-angle hook, but we are concerned about the sharp, nontapered end of such an “instrument.” Rather than improvising in this way, physicians should obtain inexpensive used and new instruments through eBay and other sources.
• Otologic alligator or micro-cup forceps. These instruments can be used to remove easily graspable objects such as paper, stickers, cotton, felt, foam, and dry flaky ear wax.
• Cyanoacrylate (superglue) on the wooden end of a cotton-tipped applicator.[9-13] This technique is recommended in cooperative patients with foreign bodies that are not easily grasped using other available tools. One author (JPL) has removed a spherical bead off the tympanic membrane using cyanoacrylate without complications. In this case there was no room for a right-angle hook and the child was cooperative. Another author (MR) has removed at least 10 objects using this technique with no complications. This technique requires that care be taken to avoid gluing the ear canal to the foreign body, the swab, or both, and that the patient remain cooperative. A small amount of glue should be applied to the wooden end of the swab and not the cotton end. The glue should be allowed to rest lightly on the foreign body for 10 seconds and then withdrawn. This technique has the advantage of appealing to some children, who find the wooden end of a cotton swab less intimidating than a metallic instrument.
Other approaches that might be considered involve using suction, applying mineral oil, or irrigating the ear canal.
• Suction. Otic suction might be used to form a vacuum seal if the foreign body is small, light, or mobile.
• Mineral oil. When a live insect is present in the ear canal mineral oil might be used. Note that this is not appropriate if perforation of the tympanic membrane is suspected.
• Irrigation. Foreign bodies that are not tightly wedged might be removed using an irrigation syringe to instill body temperature normal saline or water along the wall of the ear canal beyond the object. Note that this is not appropriate for food foreign bodies or if perforation of the tympanic membrane is suspected.
Summary
The majority of ECFB can be removed safely and effectively without referral to an otolaryngologist. However, complex cases should be referred, since they can be associated with significant morbidity, including rare incidences of tympanic membrane and ossicular damage, hearing loss (conductive or sensorineural), vertigo, or facial nerve damage.
Effective identification of high-risk cases and successful treatment of low-risk cases by ER physicians can be facilitated by adopting an individualized treatment approach. This is best based on a rational analysis of multiple variables, including patient characteristics and degree of cooperation, physician comfort and skill level, ECFB characteristics, and the availability of appropriate equipment. Repeated attempts at removal increase the risk of complications and should be undertaken with care, if at all. Because of the potentially serious consequences of failed ECFB removal in pediatric populations, referral to an otolaryngology service should be contemplated in situations involving one or more unfavorable factors for ECFB removal.
References
1. Heim SW, Maughan KL. Foreign bodies in the ear, nose, and throat. Am Fam Physician 2007;76:1185-1189.
2. Marin JR, Trainor JL. Foreign body removal from the external auditory canal in a pediatric emergency department. Pediatr Emerg Care 2006;22:630-634.
3. Singh GB, Sidhu TS, Sharma A, et al. Management of aural foreign body: An evaluative study in 738 consecutive cases. Am J Otolaryngol 2007;28:87-90.
4. DiMuzio J Jr, Deschler DG. Emergency department management of foreign bodies of the external ear canal in children. Otol Neurotol 2002;23:473-475.
5. Schulze SL, Kerschner J, Beste D. Pediatric external auditory canal foreign bodies: A review of 698 cases. Otolaryngol Head Neck Surg 2002;127:73-78.
6. Bhisitkul DM, Dunham M. An unsuspected alkaline battery foreign body presenting as malignant otitis externa. Ped Emerg Care 1992;8:141-142.
7. Premachandra DR, McRae D. Severe tissue destruction in the ear caused by alkaline button batteries. Postgrad Med J 1990;66:52-53.
8. Ludemann J. Four practical innovations which enhance quality of care in pediatric otolaryngology. Presented at the 61st Annual Meeting of the Canadian Society of Otolaryngology Head and Neck Surgery, Montreal, QC, 15 May 2007.
9. McLaughlin R, Ullah R, Heylings D. Comparative prospective study of foreign body removal from external auditory canals of cadavers with right angle hook or cyanoacrylate glue. Emerg Med J 2002;19:43-45.
10. Thompson MP. Removing objects from the external auditory canal. N Engl J Med 1984;311:1635.
11. Pride H, Schwab R. A new technique for removing foreign bodies of the external auditory canal. Pediatr Emerg Care 1989;5:135-136.
12. Benger JR, Davies PH. A useful form of glue ear. J Accid Emerg Med 2000;17:149-150.
13. Hanson RM, Stephens M. Cyanoacrylate-assisted foreign body removal from the ear and nose in children. J Paediatr Child Health 1994;30:77-78.
Mr Dance will graduate from the University of British Columbia Medical School in 2009. Dr Riley is a pediatrician in the Department of Emergency Medicine at BC Children’s Hospital and UBC. Dr Ludemann is a clinical associate professor in the Division of Otolaryngology at BCCH and UBC.